
Catheter ablation guided by three-dimensional intracardiac ultrasound in ventricular arrhythmia originating from the left posterior papillary muscle
-
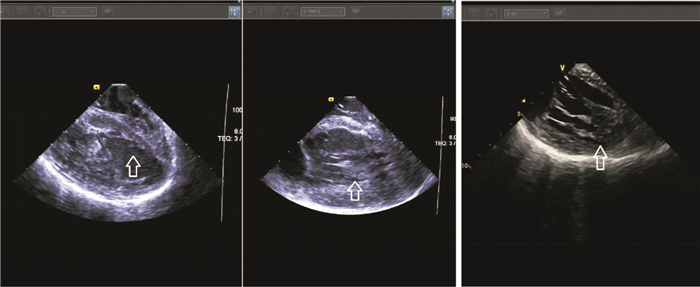
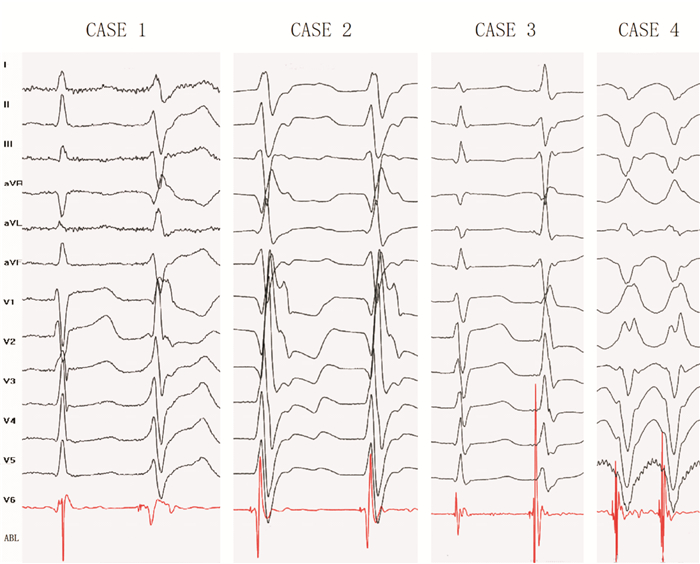
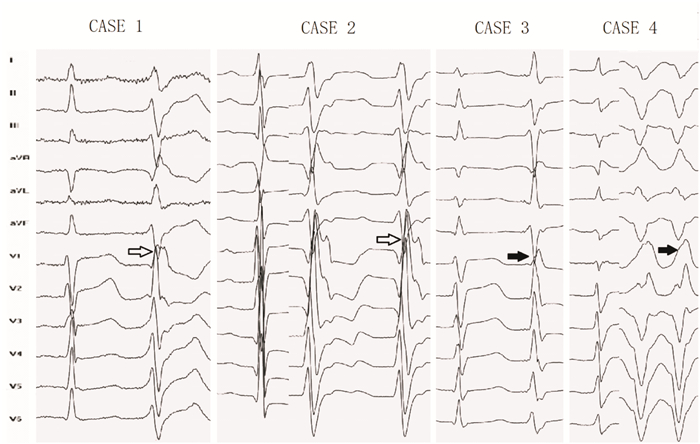
摘要: 目的 采用三维心腔内超声技术引导下,探讨起源于左心室后乳头肌的室性期前收缩和室性心动过速的电生理特征,并探讨导管消融的有效性和安全性。方法 纳入2016年7月—2020年6月收治的36例左后乳头肌起源的室性心律失常病例,常规采用三维心腔内超声技术,完成电生理标测和射频消融。统计和分析心电图和腔内电图的特征,随访12个月观察导管消融的有效性。结果 36例的体表心电图(ECG)QRS波具有相同的特征:均为右束支阻滞图形,平均时程(147±10) ms,QRS波起始段斜率较大。Ⅰ导联呈Rs型,下壁导联(Ⅱ、Ⅲ、aVF)主波以负向为主,aVR导联呈特征性的qR型,aVL导联则以正向为主。胸前导联V1~V3主波为正,而V5、V6导联可见到较深的S波。36例均成功完成标测和消融,有效消融靶点电位具有类似的特征。随访12个月无原发心律失常发作。结论 左后乳头肌起源的室性心律失常具有相似体表和腔内心电图特征。应用三维心腔内超声技术可以直视下明确定位,导管消融能够有效安全地终止该类室性心律失常发作。Abstract: Objective The purpose of this study was to investigate the electrophysiological characteristics of ventricular premature beats and ventricular tachycardia originated from the posterior papillary muscle of the left ventricle under the guidance of three-dimensional intracardiac ultrasound, and to explore the effectiveness and safety of catheter ablation.Methods Thirty-six cases of PVC/VT originating from the left ventricular posterior papillary muscles were recorded from July 2016 to June 2020 in the Central Hospital of Shengli Oil Field and The First Affiliated Hospital of Zhengzhou University. Electrophysiological mapping and radiofrequency catheter ablation(RFCA) were performed using three-dimensional intracardiac ultrasound technology. The characteristics of the body surface and intracavity electrocardiogram were analyzed. All cases were followed up for 12 months after the operation.Results The VAs of all 36 cases were successfully eliminated by catheter ablation. QRS complexes were observed with a right bundle branch block(RBBB) pattern and a steep slope in the initial segment. Lead I appeared with an Rs pattern, and inferior leads(lead Ⅱ, Ⅲ, and aVF) were usually with an S wave. The lead aVR appeared with a qR pattern, while the R wave was commonly found in aVL. The main wave in leads V1-V3 was positive but negative in V5 and V6.Conclusion VAs originating from the left ventricular posterior papillary muscles have similar electrophysiological characteristics. The origin site was accurately located using three-dimensional intracardiac ultrasound technology. Catheter ablation effectively and safely eliminated VAs.
-

-
表 1 基线特征
Table 1. Baseline characteristics
X±S 项目 LPPM组 LPF组 P值 例数 36 33 > 0.05 年龄/岁 41±16 19±17 < 0.01 男性/例(%) 21(58.3) 27(81.8) < 0.01 LVEDD/mm 49.7±6.3 48.7±3.7 0.686 左室EF/% 63.3±9.1 60.9±7.2 0.683 PVC/例(%) 28(77.8) 3(9.1) < 0.01  下载: 导出CSV
下载: 导出CSV
表 2 QRS波起始和终末70 ms电压
Table 2. Initial and terminal voltage(70 ms)of QRS waves
X±S 导联 电压/mV(起始70 ms) 电压/mV(终末70 ms) P值 Ⅰ 0.86±0.14 0.45±0.07 < 0.01 Ⅱ 1.67±0.35 0.52±0.19 < 0.01 Ⅲ 0.72±0.28 0.69±0.23 0.273 aVR 0.87±0.27 0.78±0.34 0.139 aVL 0.79±0.32 0.82±0.25 0.376 aVF 1.49±0.35 0.58±0.08 < 0.01 V1 0.76±0.27 0.62±0.17 < 0.05 V2 1.28±0.43 0.67±0.35 < 0.01 V3 1.27±0.41 0.42±0.11 < 0.01 V4 1.84±0.45 0.70±0.21 < 0.01 V5 1.96±0.54 0.66±0.22 < 0.01 V6 1.77±0.55 0.48±0.12 < 0.01
下载: 导出CSV
-
[1] Keating VP, Cooley R, Jackman WM. Anterolateral papillary muscle ventricular tachycardia[J]. Heart Rhythm, 2014, 11(5): 907-908. doi: 10.1016/j.hrthm.2013.06.006
[2] Seiler J, Lee JC, Roberts-Thomson KC, et al. Intracardiac echocardiography guided catheter ablation of incessant ventricular tachycardia from the posterior papillary muscle causing tachycardia--mediated cardiomyopathy[J]. Heart Rhythm, 2009, 6(3): 389-392. doi: 10.1016/j.hrthm.2008.11.029
[3] Chang YT, Lin YJ, Chung FP, et al. Ablation of ventricular arrhythmia originating at the papillary muscle using an automatic pacemapping module[J]. Heart Rhythm, 2016, 13(7): 1431-1440. doi: 10.1016/j.hrthm.2016.03.017
[4] Yokokawa M, Good E, Crawford T, et al. Recovery from left ventricular dysfunction after ablation of frequent premature ventricular complexes[J]. Heart Rhythm, 2013, 10(2): 172-175. doi: 10.1016/j.hrthm.2012.10.011
[5] 程宽, 陈庆兴, 庞晹, 等. 心律失常诱导的心肌病导管射频消融结果与随访[J]. 临床心血管病杂志, 2021, 37(3): 229-233. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202103009.htm
[6] Enriquez A, Supple GE, Marchlinski FE, et al. How to map and ablate papillary muscle ventricular arrhythmias[J]. Heart Rhythm, 2017, 14(11): 1721-1728. doi: 10.1016/j.hrthm.2017.06.036
[7] Farzana T, Khalil M, Mannan S, et al. Length of papillary muscles in both ventricles of different age group on Bangladeshi cadaver[J]. Mymensingh Med J, 2015, 24(1): 52-58.
[8] Al'Aref SJ, Ip JE, Markowitz SM, et al. Differentiation of papillary muscle from fascicular and mitral annular ventricular arrhythmias in patients with and without structural heart disease[J]. Circ Arrhythm Electrophysiol, 2015, 8(3): 616-624. doi: 10.1161/CIRCEP.114.002619
[9] Nogami A, Naito S, Tada H, et al. Demonstration of diastolic and presystolic Purkinje potentials as critical potentials in a macroreentry circuit of verapamil-sensitive idiopathic left ventricular tachycardia[J]. J Am Coll Cardiol, 2000, 36(3): 811-823. doi: 10.1016/S0735-1097(00)00780-4
[10] Latchamsetty R, Yokokawa M, Morady F, et al. Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes[J]. JACC Clin Electrophysiol, 2015, 1(3): 116-123. doi: 10.1016/j.jacep.2015.04.005
[11] Yamada T, Doppalapudi H, McElderry HT, et al. Electrocardiographic and electrophysiological characteristics in idiopathic ventricular arrhythmias originating from the papillary muscles in the left ventricle: relevance for catheter ablation[J]. Circ Arrhythm Electrophysiol, 2010, 3(4): 324-331. doi: 10.1161/CIRCEP.109.922310
[12] Enriquez A, Saenz LC, Rosso R, et al. Use of intracardiac echocardiography in interventional cardiology: working with the anatomy rather than fighting it[J]. Circulation, 2018, 137(21): 2278-2294. doi: 10.1161/CIRCULATIONAHA.117.031343
[13] Nishiyama T, Aizawa Y, Ito S, et al. A subtype of idiopathic ventricular fibrillation and its relevance to catheter ablation and genetic variants[J]. Heart Rhythm Case Rep, 2017, 3(5): 277-281.
[14] Muenkler P, Klatt N, Scherschel K, et al. Repolarization characteristics indicate electrical instability in ventricular arrhythmia originating from papillary muscle[J]. Europace, 2021, 23: euab116.549. doi: 10.1093/europace/euab116.549
-
图(3)
表(2)
计量
- 文章访问数: 1352
- PDF下载数: 318
- 施引文献: 0