
The application research of three-dimensional transesophageal echocardiography in transcatheter aortic valve implantation for bicuspid aortic valve stenosis patients
-
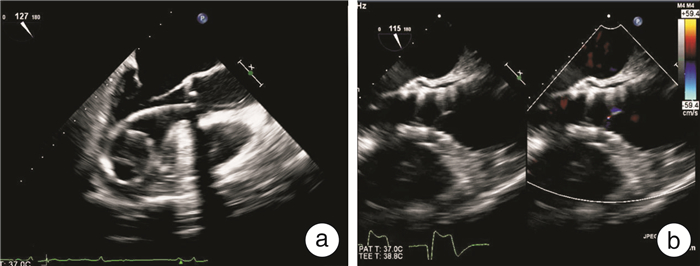
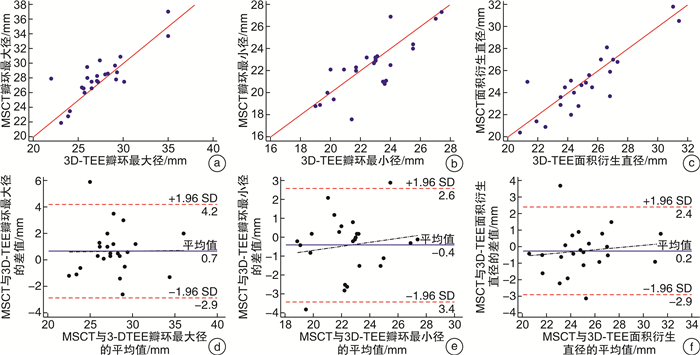
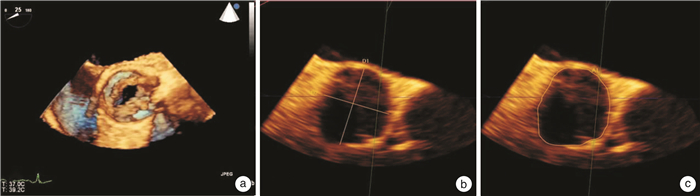
摘要: 目的 应用三维经食管超声心动图(3D-TEE)评估二叶式主动脉瓣狭窄(BAS)患者的主动脉瓣环,探讨3D-TEE指导BAS患者行经导管主动脉瓣置入术(TAVI)的可行性。方法 分析我院成功行TAVI的BAS狭窄患者24例,对术前3D-TEE与多层螺旋CT(MSCT)测量的主动脉瓣环最大径、最小径、面积及面积衍生直径进行一致性分析,根据两者面积衍生直径预测瓣膜型号,比较两者在指导人工瓣膜型号选择上的一致性。结果 3D-TEE与MSCT在测量主动脉瓣环最大径、最小径、面积、面积衍生直径方面无统计学差异(P>0.05),ICC相关系数分别为:0.817、0.781、0.885、0.869(P<0.001);3D-TEE与MSCT预测的瓣膜型号无统计学差异(P>0.05)。结论 对于二叶式主动脉瓣重度狭窄的患者,3D-TEE可为TAVI提供瓣膜型号选择,因此,在特殊情况下可作为MSCT的替代手段,帮助临床选择合适的人工瓣膜。
-
关键词:
- 二叶式主动脉瓣 /
- 经导管主动脉瓣置入术 /
- 三维经食管超声心动图 /
- 多层螺旋CT
Abstract: Objective Three-dimensional transesophageal echocardiography(3D-TEE) was applied to evaluate the aortic annulus in patients with bicuspid aortic valve stenosis(BAS). We explore the feasibility of using 3D-TEE to guide transcatheter aortic valve implantation.Methods We analyzed 24 patients with bicuspid aortic valve stenosis who successfully underwent transcatheter aortic valve implantation(TAVI) in our hospital. 3D-TEE and MSCT were used to measure the maximum diameter, minimum diameter, area and area-derived diameter of the aortic valve annulus before the operation respectively, and the results were analyzed for consistency. We compared the differences between the two methods for guiding selection of the prosthetic valve size.Results There was no significant difference between 3D-TEE and MSCT in the measurement of maximum diameter, minimum diameter, area and area-derived diameter of the aortic annulus(P > 0.05). ICC correlation coefficients were 0.817, 0.781, 0.885, 0.869(P < 0.001). There was no statistical difference in the valve size predicted by 3D-TEE and MSCT(P > 0.05).Conclusion 3D-TEE can provide guidance for artificial valve implantation in TAVI for patients with bicuspid aortic valve stenosis. -

-
表 1 TAVI术后1年与术前一般参数比较
Table 1. Comparison of conventional parameters
X±S 指标 术前 术后1年 t值 P值 主动脉瓣上最大流速/(cm·s-1) 469.79±95.35 254.54±50.98 12.205 <0.001 主动脉瓣平均跨瓣压差/mmHg1) 47.71±17.05 16.58±8.66 9.013 <0.001 左室射血分数/% 44.46±14.19 55.58±6.31 4.047 0.001 1)1 mmHg=0.133 kPa  下载: 导出CSV
下载: 导出CSV
表 2 3D-TEE与MSCT评估主动脉瓣环相关参数比较
Table 2. Aortic annulus related parameters comparison
X±S 指标 3D-TEE MSCT t值 P值 瓣环最大径/mm 27.39±3.13 28.05±3.16 1.811 0.083 瓣环最小径/mm 22.73±2.25 22.34±2.48 1.255 0.222 瓣环面积/mm2 499.63±106.83 490.71±111.33 0.849 0.404 瓣环面积衍生直径/mm 25.10±2.59 24.86±2.75 0.877 0.390
下载: 导出CSV
表 3 3D-TEE与MSCT评估主动脉瓣环大小一致性分析
Table 3. Aortic annulus correlation coefficient analysis
指标 样本例数 ICC系数(95%CI) P 瓣环最大径 24 0.817(0.627~0.915) <0.001 瓣环最小径 24 0.781(0.564~0.897) <0.001 瓣环面积 24 0.885(0.754~0.948) <0.001 瓣环面积衍生直径 24 0.869(0.723~0.940) <0.001
下载: 导出CSV
表 4 MSCT与3D-TEE预测瓣膜型号差异性比较
Table 4. Valve size comparison
例 3D-TEE MSCT 合计 符合 不符合 符合 17 1 18 不符合 2 4 6 合计 19 5 24 P=1.000
下载: 导出CSV
-
[1] He YX, Fan JQ, Zhu QF, et al. Ascending aortic dilatation rate after transcatheter aortic valve replacement in patients with bicuspid and tricuspid aortic stenosis: A multidetector computed tomography follow-up study[J]. World J Emerg Med, 2019, 10(4): 197-204. doi: 10.5847/wjem.j.1920-8642.2019.04.001
[2] 苏文华, 霍倩, 赵燕, 等. 经导管主动脉瓣植入术治疗二叶式主动脉瓣重度狭窄有效性及安全性的Meta分析[J]. 临床心血管病杂志, 2017, 33(6): 564-569. http://lcxb.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=547c0985-e98c-4197-8dd2-0fb702401f16
[3] Kanjanahattakij N, Horn B, Vutthikraivit W, et al. Comparing outcomes after transcatheter aortic valve replacement in patients with stenotic bicuspid and tricuspid aortic valve: A systematic review and meta-analysis[J]. Clin Cardiol, 2018, 41(7): 896-902. doi: 10.1002/clc.22992
[4] Wang Y, Wang M, Song G, et al. Optimal pre-TAVR annulus sizing in patients with bicuspid aortic valve: area-derived perimeter by CT is the best-correlated measure with intraoperative sizing[J]. Eur Radiol, 2019, 29(1): 259-269. doi: 10.1007/s00330-018-5592-y
[5] Kari FA, Beyersdorf F, Siepe M. Pathophysiological implications of different bicuspid aortic valve configurations[J]. Cardiol Res Pract, 2012, 2012: 735829.
[6] Zhou Q, Bi BJ, Xia ZM, et al. Application value of GE Vivid E9 Doppler echocardiography in the diagnosis of two-lobar aortic valve malformation[J]. J Integr Tradit Chin Western Med Cardio-Cerebrovasc Dis, 2019, 17(20): 3187-3189.
[7] Smith LA, Dworakowski R, Bhan A, et al. Real-time three-dimensional transesophageal echocardiography adds value to transcatheter aortic valve implantation[J]. J Am Soc Echocardiogr, 2013, 26(4): 359-369. doi: 10.1016/j.echo.2013.01.014
[8] Das R, Puri R. Transcatheter treatment of bicuspid aortic valve disease: imaging and interventional considerations[J]. Front Cardiovasc Med, 2018, 5: 91. doi: 10.3389/fcvm.2018.00091
[9] Attinger-Toller A, Bhindi R, Perlman GY, et al. Mid-term outcome in patients with bicuspid aortic valve stenosis following transcatheter aortic valve replacement with a current generation device: A multicenter study[J]. Catheter Cardiovasc Interv, 2020, 95(6): 1186-1192. doi: 10.1002/ccd.28475
[10] Kochman J, Zbroński K, Kołtowski Ł, et al. Transcatheter aortic valve implantation in patients with bicuspid aortic valve stenosis utilizing the next-generation fully retrievable and repositionable valve system: mid-term results from a prospective multicentre registry[J]. Clin Res Cardiol, 2020, 109(5): 570-580. doi: 10.1007/s00392-019-01541-8
[11] Liu X, He Y, Zhu Q, et al. Supra-annular structure assessment for self-expanding transcatheter heart valve size selection in patients with bicuspid aortic valve[J]. Catheter Cardiovasc Interv, 2018, 91(5): 986-994. doi: 10.1002/ccd.27467
[12] Xiong TY, Feng Y, Li YJ, et al. Supra-annular sizing for transcatheter aortic valve replacement candidates with bicuspid aortic valve[J]. JACC Cardiovasc Interv, 2018, 11(17): 1789-1790. doi: 10.1016/j.jcin.2018.06.002
[13] Zhao ZG, Feng Y, Liao YB, et al. Reshaping bicuspid aortic valve stenosis with an hourglass-shaped balloon for transcatheter aortic valve replacement: A pilot study[J]. Catheter Cardiovasc Interv, 2020, 95 Suppl 1: 616-623.
-
图(3)
表(4)
计量
- 文章访问数: 788
- PDF下载数: 252
- 施引文献: 0