
Influence of subclinical hypothyroidism on drug balloon interventional therapy in patients with coronary heart disease
-
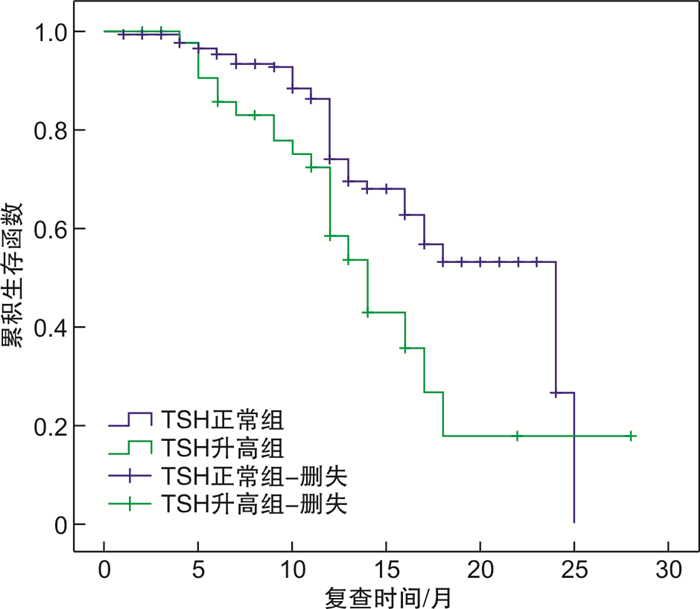
摘要: 目的 分析亚临床甲状腺功能减退症(SCH)对经皮冠状动脉(冠脉)药物球囊(DCB)介入治疗心血管事件的影响。方法 回顾性分析于2018年1月—2019年12月在阜外华中心血管病医院进行冠脉造影术确诊为冠心病并进行了DCB治疗的574例患者。按其促甲状腺激素(TSH)的含量分为两组,即482例甲状腺功能正常组(ET组)和92例SCH组。使用Kaplan-Meier生存分析,比较各组术后心血管事件(包括原位血管再次血运重建、新发血管血运重建、冠脉旁路移植、全因死亡)的差异,并使用多因素Cox回归分析术后心血管事件影响因素。结果 随访期间,ET组与SCH组原位血管再次血运重建事件(8.3% vs 20.7%,P=0.006)差异有统计学意义,生存分析(Log-rank χ2=7.091,P=0.008)两组差异具有统计学意义。多因素Cox回归分析显示,TSH是原位血管再次血运重建危险因素(HR=2.391,95%CI:1.037~5.512,P=0.041)。结论 SCH患者经皮冠脉DCB植入术后预后较差,原位血管再次血运重建事件风险明显增加。
-
关键词:
- 冠心病 /
- 亚临床甲状腺功能减退症 /
- 药物球囊
Abstract: Objective To analyze the effect of subclinical hypothyroidism(SCH) on cardiovascular events in percutaneous coronary drug balloon(DCB) interventional therapy.Methods A retrospective analysis was performed on 574 patients diagnosed with coronary heart disease by coronary angiography and treated with drug balloon in Fuwahua Central Vascular Disease Hospital from January 2018 to December 2019. According to their thyroid stimulating hormone(TSH) content, they were divided into two groups, 482 cases of normal thyroid function group(ET group) and 92 cases of SCH group. Kaplan-Meier survival analysis was used to compare the differences in postoperative cardiovascular events(including in situ revascularization, new vessel revascularization, coronary artery bypass grafting, all-cause death) between groups, and multivariate Cox regression analysis was used in postoperative cardiovascular events.Results During the follow-up period, there was a statistically significant difference in in situ vascular revascularization events between the ET group and the SCH group(8.3% vs 20.7%,P=0.006). Survival analysis(Log-rank χ2=7.091,P=0.008) showed the difference is statistically significant. Multivariate Cox regression analysis showed that TSH was a risk factor for in situ revascularization(HR=2.391, 95%CI: 1.037-5.512,P=0.041).Conclusion Patients with SCH have a poor prognosis after percutaneous coronary DCB implantation. The risk of revascularization events in situ is significantly increased.-
Key words:
- coronary heart disease /
- subclinical hypothyroidism /
- drug balloon
-

-
表 1 两组基本临床资料比较
Table 1. Basic clinical characteristics between the two groups
X±S, M(P25, P75) 项目 ET组(482例) SCH组(92例) P值 年龄/岁 59.23±11.51 61.93±11.10 0.100 男性/例(%) 371(77.0) 53(57.6) 0.001 高血压史/例(%) 284(58.9) 54(58.7) 0.968 血脂异常史/例(%) 85(17.6) 16(17.4) 0.741 PCI史/例(%) 169(35.1) 37(40.2) 0.389 糖尿病史/例(%) 161(33.4) 30(32.6) 0.882 吸烟史/例(%) 251(51.2) 33(35.9) 0.004 饮酒史/例(%) 179(37.1) 26(28.3) 0.104 身高/cm 168.0(160.0,173.0) 164.8(158.0,168.0) 0.001 体重/kg 72.0(64.3,80.0) 69.6(62.4,75.0) 0.010 BSA/(kg·m-2) 1.82±0.18 1.75±0.14 0.001 BMI/(kg·m-2) 26.4(24.2,28.9) 25.7(23.3,28.2) 0.248 术前TSH/(mIU·L-1) 2.195(1.458,2.930) 5.660(4.943,7.278) 0.001 糖化血红蛋白/% 6.0(5.6,7.1) 6.0(5.5,6.9) 0.439 总蛋白/(g·L-1) 65.5(61.4,69.2) 65.9(62.0,70.1) 0.276 HB/(mg·dL-1) 134(123,144) 120(116,139) 0.002 尿素氮/(mmol·L-1) 5.2(4.4,6.4) 4.8(4.1,6.4) 0.079 尿酸/(μmol·L-1) 306(253,377) 288(246,344) 0.172 肌酐/(μmol·L-1) 68.0(58.8,78.0) 64.0(54.0,77.8) 0.082 胆固醇/(mmol·L-1) 3.4(2.9,4.1) 3.7(3.0,4.4) 0.192 LDL-C/(mmol·L-1) 1.95(1.48,2.46) 1.83(1.45,2.54) 0.888 HDL-C/(mmol·L-1) 1.18(0.91,1.36) 1.01(0.87,1.21) 0.004 甘油三酯/(mmol·L-1) 1.33(0.96,1.94) 1.43(1.01,2.06) 0.604 术前LVEF/% 61(55,64) 61(57,65) 0.057 肾小球滤过率/% 87.11±17.95 83.24±18.10 0.139 随访TSH/(mIU·L-1) 2.230(1.490,3.050) 5.800(5.035,7.425) 0.001 PCI:经皮冠脉介入治疗;LDL-C:低密度脂蛋白胆固醇。  下载: 导出CSV
下载: 导出CSV
表 2 心血管事件发生率比较
Table 2. Comparison of incidence of cardiovascular events
例(%) 项目 ET组(482例) SCH组(92例) P值 原位血管再次血运重建 40(8.3) 19(20.7) 0.006 新发血管血运重建 22(4.6) 3(3.3) 0.759 冠脉旁路移植 2(0.4) 1(1.1) 0.519 全因死亡 1(0.2) 0(0) 0.685
下载: 导出CSV
表 3 原位血管再次血运重建影响因素的多因素Cox回归分析
Table 3. Multivariate Cox regression analysis of predictors of revascularization in situ
变量 HR(95%CI) P值 TSH 2.391(1.037~5.512) 0.041 年龄 0.985(0.948~1.023) 0.432 性别 0.912(0.377~2.206) 0.837 高血压史 0.781(0.365~1.671) 0.524 糖尿病史 1.718(0.566~5.212) 0.339 吸烟史 1.311(0.569~3.165) 0.501 甘油三酯 1.013(0.652~1.573) 0.956 HDL-C 0.458(0.122~1.716) 0.246 HB 0.983(0.965~1.002) 0.083 糖化血红蛋白 1.311(0.999~1.721) 0.051 术前LVEF 0.987(0.955~1.021) 0.454
下载: 导出CSV
表 4 患者基础疾病控制情况分析
Table 4. 患者基础疾病控制情况分析
项目 否 是 检出率/% χ2 P 血压 45.30 <0.001 术前控制是否正常 338 236 58.8 术后控制是否正常 224 350 39.0 血脂 8.06 0.005 术前控制是否正常 101 473 21.4 术后控制是否正常 67 507 13.2 血糖 52.36 <0.001 术前控制是否正常 191 379 33.3 术后控制是否正常 87 487 15.2
下载: 导出CSV
-
[1] Biondi B, Cappola AR, Cooper DS. Subclinical Hypothyroidism: A Review[J]. JAMA, 2019, 322(2): 153-160. doi: 10.1001/jama.2019.9052
[2] Delitala AP, Scuteri A, Maioli M, et al. Subclinical hypothyroidism and cardiovascular risk factors[J]. Minerva Med, 2019, 110(6): 530-545.
[3] Sue LY, Leung AM. Levothyroxine for the Treatment of Subclinical Hypothyroidism and Cardiovascular Disease[J]. Front Endocrinol(Lausanne), 2020, 11: 591588. doi: 10.3389/fendo.2020.591588
[4] Gao N, Zhang W, Zhang YZ, et al. Carotid intima-media thickness inpatients with subclinical hypothyroidism: a meta-analysis[J]. Atherosclerosis, 2013, 227: 18-25. doi: 10.1016/j.atherosclerosis.2012.10.070
[5] López-Tinoco C, Rodríguez-Mengual A, Lara-Barea A, et al. Impact of positive thyroid autoimmunity on pregnant women with subclinical hypothyroidism[J]. Endocrinol Diabetes Nutr, 2018, 65(3): 150-155. doi: 10.1016/j.endinu.2017.11.013
[6] Lee Y, Lim YH, Shin JH, et al. Impact of subclinical hypothyroidism on clinical outcomes following percutaneous coronary intervention[J]. Int J Cardiol, 2018, 253: 155-160. doi: 10.1016/j.ijcard.2017.09.192
[7] Peeters RP. Subclinical Hypothyroidism[J]. N Engl J Med, 2017, 376(26): 2556-2565. doi: 10.1056/NEJMcp1611144
[8] Fazaeli M, Khoshdel A, Shafiepour M, et al. The influence of subclinical hypothyroidism on serum lipid profile, PCSK9 levels and CD36 expression on monocytes[J]. Diabetes Metab Syndr, 2019, 13(1): 312-316. doi: 10.1016/j.dsx.2018.08.021
[9] Ma S, Jing F, Xu C, et al. Thyrotropin and obesity: increased adipose triglyceride content through glycerol-3-phosphate acyltransferase 3[J]. Sci Rep, 2015, 5: 7633. doi: 10.1038/srep07633
[10] 吴祖飞, 陈诗, 刘叶红, 等. 不同血脂成分与冠状动脉病变相关性的初步探讨[J]. 临床心血管病杂志, 2021, 37(9): 816-824. https://lcxb.chinajournal.net.cn/WKC/WebPublication/paperDigest.aspx?paperID=fdbb5a43-cd10-4461-9619-0abaeb8c859e
[11] Libby P. The changing landscape of atherosclerosis[J]. Nature, 2021, 592(7855): 524-533. doi: 10.1038/s41586-021-03392-8
[12] Iida M, Harada S, Takebayashi T. Application of metabolomics to epidemiological studies of atherosclerosis and cardiovascular disease[J]. J Atheroscler Thromb, 2019, 26(9): 747-757. doi: 10.5551/jat.RV17036
[13] Asvold BO, Bjøro T, Platou C, et al. Thyroid function and the risk of coronary heart disease: 12-year follow-up of the HUNT study in Norway[J]. Clin Endocrinol(Oxf), 2012, 77(6): 911-917. doi: 10.1111/j.1365-2265.2012.04477.x
[14] Yuan D, Zhang C, Jia S, et al. Predictive value of free triiodothyronine(FT3) to free thyroxine(FT4) ratio in long-term outcomes of euthyroid patients with three-vessel coronary artery disease[J]. Nutr Metab Cardiovasc Dis, 2021, 31(2): 579-586. doi: 10.1016/j.numecd.2020.10.011
[15] Delitala AP, Scuteri A, Maioli M, et al. Subclinical hypothyroidism and cardiovascular risk factors[J]. Minerva Med, 2019, 110(6): 530-545.
[16] Rosário P, Calsolari MR. Subclinical Hypothyroidism with TSH>7 mIU/l and≤10 mIU/l and Coronary Artery Disease[J]. Horm Metab Res, 2020, 52(2): 85-88. doi: 10.1055/a-1083-6509
[17] Wang L, Liu J, Lu K, et al. Long non-coding RNA NEAT1 regulates endothelial functions in subclinical hypothyroidism through miR-126/TRAF7 pathway[J]. Hum Cell, 2021, 34(3): 825-835. doi: 10.1007/s13577-021-00508-0
[18] Baumgartner C, da Costa BR, Collet TH, et al. Thyroid function within the normal range, subclinical hypothyroidism, and the risk of atrial fibrillation[J]. Circulation, 2017, 136(22): 2100-2116. doi: 10.1161/CIRCULATIONAHA.117.028753
[19] 时敏敏, 孟强, 张正军, 等. 促甲状腺激素对人微血管内皮细胞一氧化氮合酶的影响及其机制研究[J]. 中国医师杂志, 2018, 20(1): 64-66, 71. doi: 10.3760/cma.j.issn.1008-1372.2018.01.016
[20] Tian L, Ni J, Guo T, et al. TSH stimulates the proliferation of vascular smooth muscle cells[J]. Endocrine, 2014, 46(3): 651-658. doi: 10.1007/s12020-013-0135-4
[21] Marfella R, Ferraraccio F, Rizzo MR, et al. Innate immune activity in plaque of patients with untreated and L-thyroxine-treated subclinical hypothyroidism[J]. J Clin Endocrinol Metab, 2011, 96(4): 1015-1020. doi: 10.1210/jc.2010-1382
[22] 袁玉娟, 李吉斌, 李昊, 等. 急性心肌梗死与冠状动脉血内皮细胞源微粒、组织因子和白细胞介素-33的相关性研究[J]. 临床心血管病杂志, 2021, 37(4): 328-332. https://lcxb.chinajournal.net.cn/WKC/WebPublication/paperDigest.aspx?paperID=6d3436ef-57e5-4081-8381-bb2ff99070b6
[23] Wang L, Liu J, Lu K, et al. Long non-coding RNA NEAT1 regulates endothelial functions in subclinical hypothyroidism through miR-126/TRAF7 pathway[J]. Hum Cell, 2021, 34(3): 825-835. doi: 10.1007/s13577-021-00508-0
[24] Choi WG, Rha SW, Choi BG, et al. The Impact of Prediabetes on Two-Year Clinical Outcomes in Patients Undergoing Elective Percutaneous Coronary Intervention[J]. Yonsei Med J, 2018, 59(4): 489-494. doi: 10.3349/ymj.2018.59.4.489
[25] Redford C, Vaidya B. Subclinical hypothyroidism: Should we treat?[J]. Post Reprod Health, 2017, 23(2): 55-62. doi: 10.1177/2053369117705058
-
图(1)
表(4)
计量
- 文章访问数: 1246
- PDF下载数: 318
- 施引文献: 0