
combined therapy with ulinastatin and mucosolvan in conservative management of congenital heart disease patients with tracheal stenosis
-
摘要: 目的 探讨在心脏围手术期使用乌司他丁联合沐舒坦治疗气管狭窄是否获益。方法 回顾性分析2012年6月—2018年6月于南部战区总医院诊断为先天性心脏病(先心病)合并气管狭窄(TS)患儿42例,其中男28例,女14例;年龄1~132(17.2±13.8)个月;体重4.5~38(9.8±3.9) kg,所有患儿均未切开气道,并根据是否采用乌司他丁联合沐舒坦治疗分为治疗组22例与对照组20例。对比分析两组入监护室时气道压力峰值(Ppeak)和动脉血气分析指标、肺部感染指标、抗生素使用时间、呼吸机辅助时间和ICU时间。结果 所有心脏手术均顺利完成,全组术后死亡2例,术后14例发生肺部感染经积极治疗后均顺利恢复。全组随访29例(72.9%),随访6~72个月,平均(35±14)个月,随访期间无死亡。与对照组比较,治疗组患儿入监护室时动脉血氧分压(PaO2)和氧合指数低(OI)高,二氧化碳分压(PCO2)和乳酸(LAC)低、Ppeak低,术后再次气管插管例数少(均P<0.05),呼吸机辅助时间及ICU时间缩短(均P<0.05),抗生素使用时间较短(P<0.05)。结论 绝大多数先心病合并TS患儿可采用不切开气道保守手术方式,围手术期使用乌司他丁联合沐舒坦可加快此类患儿术后康复。Abstract: Objective To investigate whether the use of ulinastatin combined with mucosolvan in the treatment of airway stenosis during cardiac perioperative period is beneficial.Methods From June 2012 to June 2018, 42 children diagnosed congenital heart disease combined with tracheal stenosis(TS) in the Southern Theater General Hospital were retrospectively analyzed, including 28 males and 14 females, with 1-132(17.2±13.8) months old, 4.5-38(9.8±3.9) kg. No airway incision was performed in all children, and they were divided into treatment group(22 cases) and control group(20 cases). The peak airway pressure(Ppeak) and arterial blood gas analysis indicators, pulmonary infection indicators, antibiotic use time, ventilator assistance time and ICU time were compared.Results All cardiac operations were successfully completed, 2 patients died after operation in the whole group, and 14 patients suffered from pulmonary infection after operation and recovered smoothly after active treatment. Twenty-nine cases(72.9%) were followed up in the whole group for 6 to 72 months, with an average of(35±14) months. There was no death during the follow-up period. Compared with the control group, the arterial partial pressure of oxygen(PaO2) and oxygenation index(OI) were high, the partial pressure of carbon dioxide(PCO2), lactic acid(LAC), and Ppeak were low in the treatment group when they entered the intensive care unit. There were fewer cases of tracheal intubation(allP< 0.05), shorter ventilator assistance time and ICU time(allP< 0.05), and shorter antibiotic use time(P< 0.05) in treatment group.Conclusion Conservative treatment with Ulinastatin and Mucosolvan was safe and feasible for perioperative period of the majority of congenital heart disease patients with TS.
-
Key words:
- congenital heart disease /
- tracheal stenosis /
- ulinastatin /
- mucosolvan /
- conservative management
-

-

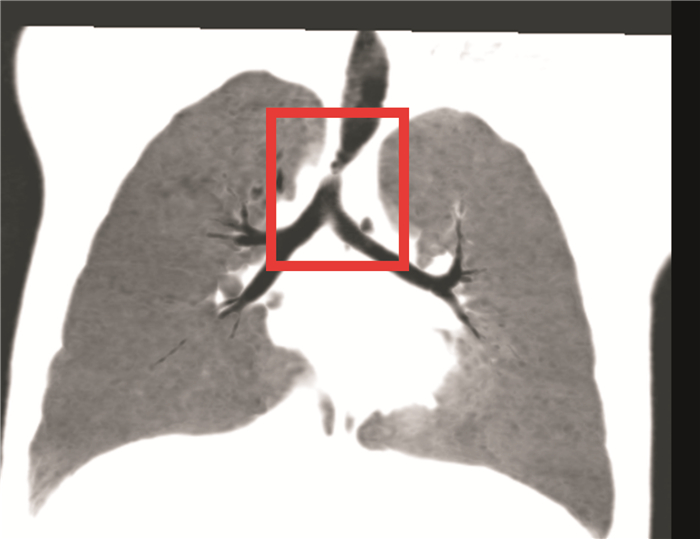
图 1 血管环压迫气管的胸部增强CT及三维重建
Figure 1. Chest CT and three-dimensional reconstruction of tracheal stenosis by vascular rings
表 1 患儿术前基本数据比较
Table 1. Patient basic data
X±S 组别 男/例(%) 年龄/月 体重/kg 简单先心/复杂先心/例 心血管畸形矫治/例 T1(Ppeak)/mH2O 气管狭窄程度/% 治疗组(22例) 12(54.5) 16.0±17.5 10.9±5.6 11/13 22 20.7±3.6 41.5±7.8 对照组(20例) 14(70.0) 18.6±19.2 9.4±4.8 7/11 20 19.8±4.1 38.2±8.6 χ2/t值 0.440 0.459 0.927 0.203 - 0.727 1.107 P值 0.507 0.649 0.359 0.653 1 0.453 0.275  下载: 导出CSV
下载: 导出CSV
表 2 患儿血气及氧合指标分析
Table 2. Early postoperative blood gas and oxygenation indexes
X±S 组别 PaO2/mmHg PaCO2/mmHg 氧合指数 LAC/(mmol·L-1) T2(Ppeak)/cmH2O 治疗组(21例) 177.0±35.8 39.6±7.4 430.2±39.2 0.9±0.7 22.8±7.1 对照组(19例) 155.9±26.3 44.6±6.3 393.4±38.6 1.5±1.0 28.8±8.6 t值 2.105 2.289 2.987 2.216 2.42 P 0.042 0.028 0.005 0.033 0.021
下载: 导出CSV
表 3 患儿感染相关指标分析
Table 3. Postoperative infection related indexes
X±S 组别 WBC/(×109·L-1) PCT/(μg·L-1) CRP/(mg·L-1) 肺部感染/例(%) 治疗组(21例) 11.2±4.8 0.34±0.20 63.5±18.2 6(28.6) 对照组(19例) 11.5±4.4 0.39±0.25 62.3±20.5 8(42.1) χ2/t值 0.205 0.702 0.196 0.803 P值 0.838 0.487 0.846 0.370
下载: 导出CSV
表 4 患儿术后一般数据比较
Table 4. Early postoperative clinical data
X±S 组别 机械通气时间/h ICU时间/h 抗生素使用时间/d 多次气管插管/例(%) 治疗组(21例) 37.8±11.1 58.8±5.1 9.1±3.3 3(14.3) 对照组(19例) 48.1±19.8 63.6±6.8 11.9±4.8 8(42.1) χ2/t值 2.056 2.541 2.168 3.872 P值 0.047 0.015 0.037 0.049
下载: 导出CSV
-
[1] Parental risk factors associated with congenital heart disease in a Thai population: multivariable analysis[J]. Asian Biomed, 2021, 15(6): 267-276.
[2] Yubbu P, Abdul Latiff H, Musa H, et al. Cardiovascular causes of tracheobronchial compression: a decade experience in a Paediatric Congenital Heart Centre[J]. Cardiol Young, 2022, 32(3): 374-382. doi: 10.1017/S1047951121002110
[3] 刘慧, 刘晓燕. 先天性心脏病合并气道异常患儿的临床分析[J]. 中国循证儿科杂志, 2015, 10(5): 345-349. https://www.cnki.com.cn/Article/CJFDTOTAL-XZEK201505009.htm
[4] 王旭, 李守军, 段雷雷, 等. 先天性心脏病合并气管狭窄的保守治疗策略[J]. 中国分子心脏病学杂志, 2012, 12(1): 12-14. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGFB201201006.htm
[5] 邸勇, 王葵亮, 曹倩, 等. 保守插管策略在先天性心脏病合并气管狭窄患儿术中的应用[J]. 临床麻醉学杂志, 2017, 33(2): 179-180. https://www.cnki.com.cn/Article/CJFDTOTAL-LCMZ201702025.htm
[6] Guo K, Tan Q. Observation on the clinical efficacy of mucosolvan aerosol inhalation combined with intravenous drip in the treatment of neonatal pneumonia[J]. Clin Med Enginee, 2019, 110: 50.
[7] Zhang R, Ma J, Zheng P, et al. Ulinastatin plus biapenem for severe pneumonia in the elderly and its influence on pulmonary function and inflammatory cytokines[J]. Am J Transl Res, 2021, 13(5): 5027-5034.
[8] Xi S, Le H, Wu H, et al. The Protection Effect of Ulinastatin on Freshwater Instillation-Induced Acute Lung Injury in Rabbits[J]. Heart, 2020, 110: 50.
[9] Xiong S, Guo W, Ren Z, et al. Effects and mechanisms of drug-loaded ulinastatin nanoparticles on inflammatory response in sepsis[J]. Sci Adv Mater, 2021, 13(3): 481-489. doi: 10.1166/sam.2021.3954
[10] 于浩, 颜涛, 马涛, 等. 乌司他丁对复杂先天性心脏病患儿体外循环围术期肺保护作用的研究[J]. 广东医学, 2017, 38(20): 3184-3187. doi: 10.3969/j.issn.1001-9448.2017.20.033
[11] 王荣品, 梁长虹, 黄美萍, 等. 儿童先天性心脏病伴气管支气管狭窄的多层螺旋CT诊断[J]. 中华放射学杂志, 2010, 44(8): 811-815. doi: 10.3760/cma.j.issn.1005-1201.2010.08.006
[12] 王红阳, 张庆, 郭纪全. 呼吸内科疾病诊断标准[M]. 北京, 人卫, 2009: 110.
[13] Coln E, Carrasco J, Coln D. Demonstrating relief of cardiac compression with the Nuss minimally invasive repair for pectus excavatum[J]. J Pediatr Surg, 2006, 41(4): 683-686;discussion 683-6. doi: 10.1016/j.jpedsurg.2005.12.009
[14] 殷勇, 肖洁, 岳孟源, 等. 先天性心脏病合并气管狭窄的诊治策略[J]. 复旦学报(医学版), 2005, 32(2): 159-160. https://www.cnki.com.cn/Article/CJFDTOTAL-SHYK200502008.htm
[15] Hou Q, Gao W, Zhong Y, et al. Diagnostic Accuracy of Three-dimensional Turbo Field Echo Magnetic Resonance Imaging Sequence in Pediatric Tracheobronchial Anomalies with Congenital Heart Disease[J]. Sci Rep, 2018, 8(1): 2529. doi: 10.1038/s41598-018-20892-2
[16] Green GE, Ohye RG. Diagnosis and management of tracheal anomalies and tracheal stenosis-science direct[J]. Heart, 2021, 110: 50.
[17] 黄杏玲, 邓新娥, 王远流, 等. 不同类型胎儿先天性心脏病的产前诊断及预后分析[J]. 实用医学杂志, 2020, 36(21): 2990-2994. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYZ202021021.htm
[18] 孙欣彤, 崔晓霈, 解辉, 等. 山东省单中心肺动脉高压患者社会支持情况与诊疗依从性调查研究[J]. 临床心血管病杂志, 2022, 38(2): 146-151. https://lcxb.chinajournal.net.cn/WKC/WebPublication/paperDigest.aspx?paperID=969a180d-db4f-42c5-b702-cc93a3f65d05
[19] 向军, 何玲, 舒凯森, 等. 儿童先天性心脏病术后低心排综合征的危险因素分析[J]. 临床心血管病杂志, 2020, 36(6): 554-558. https://lcxb.chinajournal.net.cn/WKC/WebPublication/paperDigest.aspx?paperID=d845ee5c-0862-44b4-b6f6-537b283b0350
[20] 陈小莉, 魏利娟, 郭仲辉, 等. 压力控制容量保证用于婴幼儿先天性心脏病术中肺保护性通气的效果[J]. 实用医学杂志, 2020, 36(4): 470-474. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYZ202004011.htm
[21] 王志岭, 王洁. 乌司他丁灌注对先天性心脏病患者体外循环后肺功能、炎症因子的影响[J]. 临床研究, 2020, 28(6): 29-30. https://www.cnki.com.cn/Article/CJFDTOTAL-LCYN202006013.htm
[22] 蔡治祥, 王显悦, 颜涛, 等. 自体肺动脉补片和扩大端端/端侧术矫治婴幼儿主动脉缩窄疗效分析[J]. 临床心血管病杂志, 2018, 34(8): 797-802. https://lcxb.chinajournal.net.cn/WKC/WebPublication/paperDigest.aspx?paperID=cae0adc9-90c0-49ce-b81e-e0b0728629a2
-
图(2)
表(4)
计量
- 文章访问数: 1088
- PDF下载数: 297
- 施引文献: 0