
Risk factors of out-of hospital pericardial effusion after left atrial appendage closure
-
摘要: 目的 探讨左心耳和毗邻结构的距离以及术后心律与左心耳封堵(left atrial appendage closure,LAAC)术后院外心包积液(out-of-hospital pericardial effusion,OHPE)的关系。方法 回顾性纳入2015年5月—2019年5月于南方医科大学南方医院行LAAC的52例患者,其中发生OHPE 12例纳入OHPE组,余40例纳入对照组。利用心血管造影计算机断层扫描(cardiac computed tomography angiography,cCTA)评估左心耳与毗邻结构,包括肺动脉(pulmonary artery,PA)、左上肺静脉(left superior pulmonary vein,LSPV)、左冠状动脉回旋支(left circumflex coronary artery,LCX)的距离。采用多因素logistic回归分析LAAC术后发生OHPE的危险因素,并利用受试者工作特征曲线(receiver operating characteristic curve,ROC)分析危险因素对OHPE的诊断价值。结果 与对照组比较,OHPE组左心耳与PA、LSPV的距离明显减小[PA:(3.6±1.5) mm vs (2.5±1.3) mm,P=0.006;LSPV:(3.2±1.4) mm vs (2.6±1.9) mm,P=0.025];两组左心耳与LCX的距离差异无统计学意义(P=0.157)。多因素回归分析显示,左心耳与PA的距离是LAAC术后发生OHPE的独立保护因素(OR=0.466,95%CI:0.234~0.927,P=0.030)。左心耳与PA的距离预测OHPE的ROC曲线下面积为0.765(95%CI:0.626~0.871,P < 0.01),最佳预测值为2 mm,特异度为90.0%,灵敏度为58.3%。此外,转复窦性心律的患者更易发生OHPE(OR=7.071,95%CI:1.124~44.506,P=0.037)。结论 左心耳与PA的距离可作为LAAC术后OHPE的预测指标,转复窦性心律的患者更容易发生OHPE。Abstract: Objective To explore the relationship between the distance from the left atrial appendage to neighboring structures, postoperative heart rhythm, and out-of-hospital pericardial effusion(OHPE) after left atrial appendage closure(LAAC).Methods Fifty-two patients who underwent LAAC at Southern Hospital of Southern Medical University from May 2015 to May 2019 were retrospectively included, 12 cases with OHPE were included in the OHPE group, and the other 40 cases were included in the control group. Cardiac computed tomography angiography(cCTA) was used to measure the distance from the left atrial appendage to neighboring structures, including the pulmonary artery(PA), left superior pulmonary vein(LSPV), and left circumflex coronary artery(LCX). Logistic regression analysis was used to identify risk factors of OHPE after LAAC, and the receiver operating characteristic curve(ROC) was used to analyze the diagnostic value of risk factors for OHPE.Results Compared with the control group, the distance from the left atrial appendage to PA and LSPV in the OHPE group was significantly shorter(PA: [3.6±1.5]mm vs[2.5±1.3]mm, P=0.006; LSPV: [3.2±1.4]mm vs[2.6±1.9]mm, P=0.025); There was no statistically significant difference in the distance from the left atrial appendage to LCX between the two groups(P=0.157). Logistic regression analysis showed that the distance from the left atrial appendage to PA was an independent protective factor for OHPE(OR=0.466, 95%CI: 0.234-0.927, P=0.030). ROC analysis revealed that the area under the ROC curve of OHPE predicted by the distance from the left atrial appendage to PA was 0.765(95%CI: 0.626-0.871, P < 0.01), the cut-off value was 2 mm, the specificity was 90.0%, and the sensitivity was 58.3%. Otherwise, patients who converted to sinus rhythm were more likely to develop OHPE(OR=7.071, 95%CI: 1.124-44.506, P=0.037).Conclusion The distance from the left atrial appendage to PA can be used as a predictor of OHPE after LAAC. Patients who converted to sinus rhythm are more likely to develop OHPE.
-

-
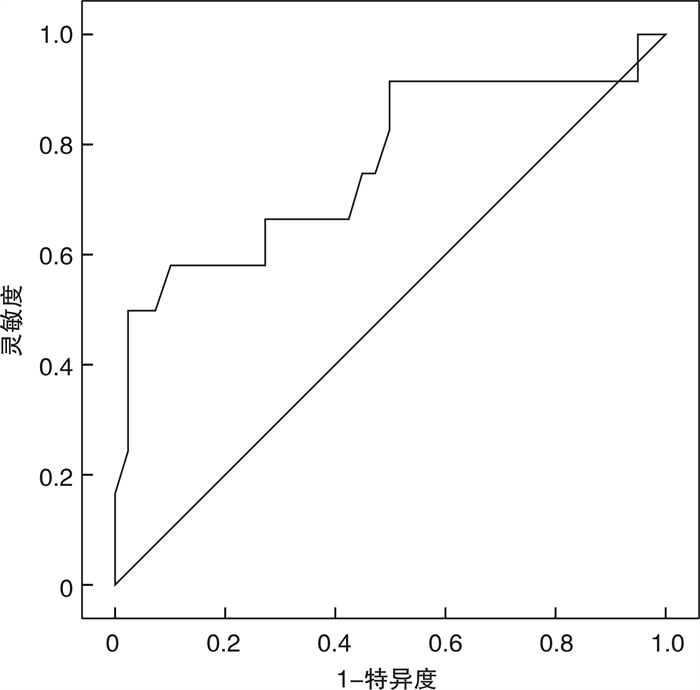
图 1 左心耳与PA的距离预测OHPE的ROC曲线
Figure 1. The ROC curve of OHPE predicted by the distance from left atrial appendage to PA
表 1 研究对象的临床基线资料
Table 1. Clinical baseline data
例(%), X±S 项目 整体(52例) 对照组(40例) OHPE组(12例) P 年龄/岁 66.7±8.3 66.4±8.2 67.6±9.3 0.671 男性 33(63.5) 23(57.5) 10(83.3) 0.198 BMI/(kg/m2) 24.9±4.3 24.8±4.1 25.0±5.1 0.872 高血压 36(69.2) 26(65.0) 10(83.3) 0.395 糖尿病 8(15.4) 4(10.0) 4(33.3) 0.131 CHA2DS2-VASc评分 4.4±1.8 4.3±1.7 4.8±2.1 0.412 HAS-BLED评分 2.0±1.1 2.0±1.0 1.9±1.2 0.991 左心室射血分数/% 59.5±8.0 60.4±7.1 56.6±10.4 0.154 左心房内径/mm 44.7±6.7 44.4±6.2 45.6±8.5 0.312 NYHA分级 1.000 Ⅰ 10(19.2) 8(20.0) 2(16.7) Ⅱ 39(75.0) 30(75.0) 9(75.0) Ⅲ 3(5.8) 2(5.0) 1(8.3) 房颤类型 0.811 阵发性 18(34.6) 13(32.5) 5(41.7) 持续性 34(65.4) 27(67.5) 7(58.3) 封堵器类型 0.565 盖子式 16(30.8) 11(27.5) 5(41.7) 塞子式 36(69.2) 29(72.5) 7(58.3) 封堵器尺寸/mm 28.8±3.7 29.0±3.5 28.3±4.3 0.566 左心耳类型 0.212 仙人掌型 11(21.2) 10(25.0) 1(8.3) 鸡翅型 16(30.8) 14(35.0) 2(16.7) 风向标型 10(19.2) 7(17.5) 3(25.0) 菜花型 15(28.8) 9(22.5) 6(50.0) cCTA测量值/mm 左心耳开口长轴 28.9±3.8 29.4±3.5 27.2±4.5 0.089 左心耳开口短轴 22.2±4.8 22.6±4.5 20.6±5.5 0.193 术式 0.321 一站式手术 40(76.9) 29(72.5) 11(91.7) 仅左心耳封堵 12(23.1) 11(27.5) 1(8.3)  下载: 导出CSV
下载: 导出CSV
表 2 对照组与OHPE组左心耳毗邻结构的距离
Table 2. The distance from the left atrial appendage to adjacent structures
mm, X±S 组别 左心耳与PA距离 左心耳与LSPV距离 左心耳与LCX距离 对照组(40例) 3.6±1.5 3.2±1.4 2.9±1.5 OHPE组(12例) 2.5±1.3 2.6±1.9 3.4±1.2 P 0.006 0.025 0.157
下载: 导出CSV
表 3 OHPE危险因素的logistic回归分析
Table 3. Risk factors of OHPE analyzed by logistic analysis
项目 单因素 多因素 OR 95%CI P OR 95%CI P 糖尿病 4.500 0.924~21.925 0.063 4.639 0.779~27.619 0.092 左心耳与PA距离 0.463 0.236~0.907 0.025 0.466 0.234~0.927 0.030
下载: 导出CSV
-
[1] Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery(EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology(ESC)Developed with the special contribution of the European Heart Rhythm Association(EHRA)of the ESC[J]. Eur Heart J, 2021, 42(5): 373-498. doi: 10.1093/eurheartj/ehaa612
[2] Beigel R, Wunderlich NC, Ho, SY, et al. The left atrial appendage: anatomy, function, and noninvasive evaluation[J]. JACC Cardiovasc Imaging, 2014, 7(12), 1251-1265.
[3] 庞乃栋, 张楠, 郭敏, 等. 左心耳电隔离在持续性心房颤动治疗中的研究进展[J]. 临床心血管病杂志, 2022, 38(1): 6-10. doi: 10.13201/j.issn.1001-1439.2022.01.002 https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.01.002
[4] Reddy VY, Doshi SK, Kar S, et al. 5-Year Outcomes After Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials[J]. J Am Coll Cardiol, 2017, 70(24): 2964-2975. doi: 10.1016/j.jacc.2017.10.021
[5] Landmesser U, Schmidt B, Nielsen-Kudsk JE, et al. Left atrial appendage occlusion with the AMPLATZER Amulet device: periprocedural and early clinical/echocardiographic data from a global prospective observational study[J]. EuroIntervention, 2017, 13(7): 867-876. doi: 10.4244/EIJ-D-17-00493
[6] Huang H, Liu Y, Xu Y, et al. Percutaneous Left Atrial Appendage Closure With the LAmbre Device for Stroke Prevention in Atrial Fibrillation: A Prospective, Multicenter Clinical Study[J]. JACC Cardiovasc Interv, 2017, 10(21): 2188-2194. doi: 10.1016/j.jcin.2017.06.072
[7] Yang L, Zhang X, Jin Q, et al. Pericardial Effusion During the Perioperative Period for Left Atrial Appendage Closure[J]. Front Cardiovasc Med, 2021, 8: 678460. doi: 10.3389/fcvm.2021.678460
[8] Munir MB, Khan MZ, Darden D, et al. Pericardial effusion requiring intervention in patients undergoing percutaneous left atrial appendage occlusion: Prevalence, predictors, and associated in-hospital adverse events from 17, 700 procedures in the United States[J]. Heart Rhythm, 2021, 18(9): 1508-1515. doi: 10.1016/j.hrthm.2021.05.017
[9] Price MJ, Valderrábano M, Zimmerman S, et al. Periprocedural Pericardial Effusion Complicating Transcatheter Left Atrial Appendage Occlusion: A Report From the NCDR LAAO Registry[J]. Circ Cardiovasc Interv, 2022, 15(5): e011718.
[10] Liu B, Luo J, Gong M, et al. Five-Year Outcomes and Cardiac Remodeling Following Left Atrial Appendage Occlusion[J]. Clin Interv Aging, 2021, 16: 655-663. doi: 10.2147/CIA.S296639
[11] 段文涛, 张峰, 陈萍, 等. CT血管造影成像与超声心动图在预测非瓣膜性心房颤动患者左心耳血栓形成中的应用[J]. 临床心血管病杂志, 2023, 39(3): 201-207. doi: 10.13201/j.issn.1001-1439.2023.03.009 https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2023.03.009
[12] Korsholm K, Berti S, Iriart X, et al. Expert Recommendations on Cardiac Computed Tomography for Planning Transcatheter Left Atrial Appendage Occlusion[J]. JACC Cardiovasc Interv, 2020, 13(3): 277-292. doi: 10.1016/j.jcin.2019.08.054
[13] Hanazawa K, Brunelli M, Saenger J, et al. Close proximity between pulmonary artery and left atrial appendage leading to perforation of the artery, tamponade and death after appendage closure using cardiac plug device[J]. Int J Cardiol, 2014, 175(2): e35-6. doi: 10.1016/j.ijcard.2014.04.260
[14] Xiao F, Chen Y, Chen Y, et al. Delayed pericardial effusion after left atrial appendage closure with the LAmbre device: Importance of a fully open umbrella[J]. J Cardiovasc Electrophysiol, 2021, 32(6): 1646-1654. doi: 10.1111/jce.15020
[15] Demkow M, Konka M, Witkowski A, et al. How to Prevent Pulmonary Artery Wall Perforation Following Transcatheter Occlusion of Left Atrial Appendage[J]. J Am Soc Echocardiogr, 2021, 34(2): 195-197. doi: 10.1016/j.echo.2020.10.010
[16] Halkin A, Cohen C, Rosso R, et al. Left atrial appendage and pulmonary artery anatomic relationship by cardiac-gated computed tomography: Implications for late pulmonary artery perforation by left atrial appendage closure devices[J]. Heart Rhythm, 2016, 13(10): 2064-2069. doi: 10.1016/j.hrthm.2016.07.015
[17] Zou T, Chen Q, Zhang L, et al. Pulmonary artery pressure is associated with mid-term major adverse cardiovascular events and postprocedure pericardial effusion in atrial fibrillation patients undergoing left atrial appendage occlusion[J]. Ann Transl Med, 2021, 9(16): 1324. doi: 10.21037/atm-21-3561
[18] Kulawiak-Gałąska DA, Gałąska R, Mielczarek M, et al. Pulmonary artery and left atrial appendage anatomical relationship using electrocardiogram——gated computed tomography: An important aspect of left atrial appendage occlusion[J]. Cardiol J, 2021, 28(2): 342-344. doi: 10.5603/CJ.a2021.0024
[19] Li CY, Gao BL, Liu XW, et al. Quantitative Evaluation of the Substantially Variable Morphology and Function of the Left Atrial Appendage and Its Relation with Adjacent Structures[J]. PLoS One, 2015, 10(7): e0126818. doi: 10.1371/journal.pone.0126818
[20] Chun KR, Bordignon S, Urban V, et al. Left atrial appendage closure followed by 6 weeks of antithrombotic therapy: a prospective single-center experience[J]. Heart Rhythm, 2013, 10(12): 1792-179. doi: 10.1016/j.hrthm.2013.08.025
[21] 杨再鑫, 石亮, 王彦江, 等. 心房颤动射频消融术中活化凝血时间维持在220~270 s的安全性[J]. 临床心血管病杂志, 2022, 38(6): 467-471. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.06.008
-
图(1)
表(3)
计量
- 文章访问数: 1085
- PDF下载数: 192
- 施引文献: 0