
Predictive value of homocysteine combined with neutrophils for myocardial no-reflow in postmenopausal women
-
摘要: 目的 探讨血同型半胱氨酸(Hcy)和中性粒细胞计数(ANC)对绝经后急性ST段抬高型心肌梗死(STEMI)患者经皮冠状动脉介入治疗(PCI)术中无复流的预测价值。 方法 回顾性选择绝经后首诊STEMI并于2017年12月—2019年10月在宁夏医科大学总医院接受急诊PCI治疗的126例患者,根据冠状动脉(冠脉)造影结果分为正常血流组(95例)和无复流组(31例)。比较两组基线资料,应用logistic回归分析评估Hcy和ANC对绝经后STEMI患者PCI术中无复流的影响。通过ROC曲线评估Hcy联合ANC对心肌无复流的预测价值。 结果 纳入患者126例,无复流发生率为24.66%。多因素logistic回归显示,术前Hcy(OR=1.136,95%CI:1.067~1.210,P<0.001)和ANC(OR=1.280,95%CI:1.091~1.501,P=0.002)是无复流发生的危险因素。ROC曲线分析显示,ANC预测心肌无复流的曲线下面积为0.724(95%CI:0.619~0.829),截断值为9.88×109/L,灵敏度为64.5%,特异度为81.1%;Hcy预测心肌无复流的曲线下面积为0.783(95%CI:0.683~0.884),截断值为20.04 μmol/L,灵敏度为67.7%,特异度为83.2%;Hcy联合ANC预测心肌无复流的曲线下面积为0.838(95%CI:0.753~0.922),灵敏度为90.3%,特异度为76.3%。 结论 Hcy≥20.04 μmol/L联合ANC≥9.88×109/L可用于预测绝经后STEMI患者PCI术中无复流的发生风险,具有较强的预测价值。
-
关键词:
- 同型半胱氨酸 /
- 中性粒细胞 /
- 绝经 /
- 无复流 /
- ST段抬高型心肌梗死
Abstract: Objective To investigate the predictive value of blood homocysteine(Hcy) and neutrophils counts(ANC) for no-reflow during percutaneous coronary intervention(PCI) in postmenopausal patients with ST-segment elevation myocardial infarction(STEMI). Methods A total of 126 postmenopausal patients with first-episode STEMI underwent emergency PCI in the General Hospital of Ningxia Medical University from December 2017 to October 2019 were enrolled. According to coronary angiography results, they were divided into the normal flow group(n=95) and the no-reflow group(n=31). Baseline data were compared between the two groups. Logistic regression model was used to analyze the independent factors of no-reflow, and ROC curves were performed to assess the predictive efficacy of Hcy and ANC. Results The incidence of NRP was 24.6% in 126 included patients. After adjusting for confounding factors, logistic regression showed that Hcy(OR=1.136, 95%CI: 1.067-1.210, P < 0.001) and ANC(OR=1.280, 95%CI: 1.091-1.501, P=0.002) were independent predictors of no-reflow. ROC analysis showed that the area under the ROC curve(AUC) for predicting myocardial no-reflow by ANC was 0.724(95%CI: 0.619-0.829), with a cutoff value of 9.88×109/L, sensitivity of 64.5%, and specificity of 81.1%; The AUC for predicting myocardial no-reflow by HCY was 0.783(95%CI: 0.683-0.884), with a cutoff value of 20.04 μmol/L, sensitivity of 67.7%, and specificity of 83.2%; The AUC of Hcy combined with ANC for predicting myocardial no-reflow was 0.838(95%CI: 0.753-0.922), with a sensitivity of 90.3%, specificity of 76.3%. Conclusion Hcy≥20.04 μmol/l and ANC counts≥9.88×109/L can be used to predict the risk of no-reflow during PCI in postmenopausal STEMI patients, and has high predictive value.-
Key words:
- homocysteine /
- neutrophils /
- menopause /
- no-reflow /
- acute ST-segment elevation myocardial infarction
-

-
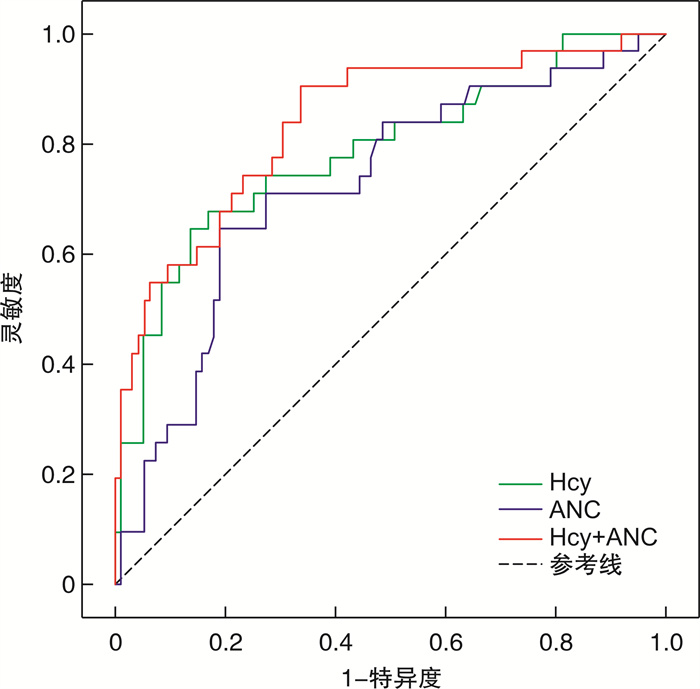
图 1 Hcy、ANC和Hcy联合ANC预测无复流的ROC曲线分析
Figure 1. ROC curves of Hcy, ANC and Hcy combined with ANC for prediction of no-reflow
表 1 两组基线数据比较
Table 1. Comparison of baseline dates between two groups
例(%), X±S 项目 血流正常组(95例) 无复流组(31例) χ2/t P 年龄/岁 69.22±9.31 68.74±9.75 -0.246 0.806 高血压病 60(63.18) 21(67.74) 0.214 0.644 糖尿病 32(33.68) 12(38.71) 0.260 0.610 血脂异常 21(22.11) 10(32.26) 0.274 0.601 吸烟史 7(7.37) 0 2.419 0.120 冠心病家族史 12(12.63) 6(19.35) 0.863 0.353 BMI/(kg/m2) 23.01±3.37 23.09±3.41 0.114 0.910 入院心率/(次/min) 79.68±13.45 86.23±15.58 2.172 0.032 入院SBP/mmHg 119.97±22.28 111.29±19.87 -1.931 0.056 入院DBP/mmHg 73.78±13.03 70.29±15.55 -1.244 0.216 入院Killip分级 0.411 0.521 Ⅰ级 70(73.68) 21(67.74) Ⅱ~Ⅳ级 25(26.32) 10(32.26)  下载: 导出CSV
下载: 导出CSV
表 2 两组检验及心脏超声相关数据比较
Table 2. Comparison of baseline characteristics between two groups
X±S 项目 血流正常组(95例) 无复流组(31例) t P Hcy/(μmol/L) 16.71±6.69 29.14±15.63 6.230 0.000 肌酐/(μmol/L) 56.81±15.20 73.53±24.32 3.168 0.002 白细胞计数/(×109/L) 9.95±3.01 12.37±3.73 3.648 0.000 ANC/(×109/L) 8.14±2.95 10.58±3.59 3.777 0.000 淋巴细胞计数/(×109/L) 1.31±0.75 1.23±0.57 -0.540 0.590 单核细胞计数/(×109/L) 0.44±0.24 0.53±0.28 1.729 0.086 C反应蛋白/(mg/L) 11.51±2.07 16.35±2.51 1.057 0.292 血红蛋白/(g/L) 127.43±14.01 123.55±14.33 -1.333 0.185 血小板计数/(×109/L) 246.27±87.76 237.97±56.75 0.124 0.622 白蛋白/(g/L) 38.54±5.09 37.06±4.75 -1.432 0.155 TG /(mmol/L) 1.71±0.16 1.57±0.79 -0.605 0.547 TC /(mmol/L) 4.37±0.97 4.44±1.07 0.299 0.765 LDL-C/(mmol/L) 2.25±0.73 2.28±0.88 0.218 0.828 HDL-C/(mmol/L) 1.03±0.31 1.03±0.20 0.020 0.984 肌钙蛋白I/(ng/mL) 27.6±8.54 26.53±3.55 0.188 0.851 NT-proBNP/(pg/mL) 1 098.94±16.18 1 347.73±19.45 -0.713 0.477 LVEF/% 50.69±9.35 49.85±8.68 -0.442 0.659
下载: 导出CSV
表 3 两组介入相关数据比较
Table 3. Comparison of PCI-related data between two groups
例(%), X±S 变量 血流正常组(95例) 无复流组(31例) χ2/t P 病变血管数量 0.411 0.521 1支 25(26.32) 10(32.26) >1支 70(73.68) 21(67.74) 术前TIMI血流 0.526 0.408 0~1级 88(92.63) 30(96.77) 2~3级 7(7.37) 1(3.23) 梗死相关动脉 LAD 46(48.42) 14(45.16) 0.100 0.752 LCX 43(45.26) 11(35.48) 4.032 0.045 RCA 6(6.32) 6(19.35) 0.913 0.339 IABP 4(4.21) 8(25.81) 12.651 0.000 胸痛至导丝通过时间/h 7.07±2.76 7.40±2.51 -0.596 0.553 胸痛至药物服用时间/h 3.21±1.25 3.68±1.34 -1.707 0.091 支架数量/个 1.55±0.74 1.32±0.54 -1.558 0.122 支架直径/mm 4.88±0.37 3.81±0.59 1.289 0.200 支架长度/mm 23.87±9.34 26.31±8.61 -0.772 0.441
下载: 导出CSV
表 4 无复流影响因素的单因素logistic回归分析
Table 4. The influencing factors of no-reflow analyzed by univariate logistic analysis
变量 B S.E. Wald OR 95%CI P 心率 0.029 0.014 4.384 1.029 1.002~1.057 0.036 Hcy 0.116 0.028 17.402 1.123 1.064~1.186 <0.001 肌酐 0.024 0.010 6.407 1.025 1.006~1.044 0.011 WBC 0.210 0.066 10.149 1.234 1.084~1.404 0.001 ANC 0.225 0.069 10.682 1.252 1.094~1.433 0.001 LCX -1.270 0.620 4.192 0.281 0.083~0.947 0.041 IABP -2.069 0.612 1.281 0.126 0.035~0.457 0.002
下载: 导出CSV
表 5 无复流的多因素logistic回归分析
Table 5. The influencing factors of no-reflow analyzed by multivariate logistic
变量 B S.E. Wald OR 95%CI P Hcy 0.127 0.032 15.726 1.136 1.067~1.210 <0.001 ANC 0.247 0.081 9.206 1.280 1.091~1.501 0.002
下载: 导出CSV
-
[1] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2020概要[J]. 中国循环杂志, 2021, 36(6): 521-545. doi: 10.3969/j.issn.1000-3614.2021.06.001
[2] Ing CT, Ahn HJ, Kawakami R, et al. Ethnic and Gender Differences in 10-Year Coronary Heart Disease Risk: a Cross-Sectional Study in Hawai'i[J]. J Racial Ethn Health Disparities, 2021, 8(4): 943-952. doi: 10.1007/s40615-020-00851-2
[3] Pantea-Roşan LR, Pantea VA, Bungau S, et al. No-Reflow after PPCI-A Predictor of Short-Term Outcomes in STEMI Patients[J]. J Clin Med, 2020, 9(9): 2956. doi: 10.3390/jcm9092956
[4] Yang L, Cong H, Lu Y, et al. A nomogram for predicting the risk of no-reflow after primary percutaneous coronary intervention in elderly patients with ST-segment elevation myocardial infarction[J]. Ann Transl Med, 2021, 9(2): 126. doi: 10.21037/atm-20-8003
[5] 董海秋, 董梅, 任法新. 绝经后内源性雌激素水平与急性ST段抬高型心肌梗死患者心肌再灌注后无复流的关系[J]. 中国循环杂志, 2017, 32(6): 552-555. doi: 10.3969/j.issn.1000-3614.2017.06.006
[6] Marjoribanks J, Farquhar CM, Roberts H, et al. Cochrane corner: long-term hormone therapy for perimenopausal and postmenopausal women[J]. Heart, 2018, 104(2): 93-95. doi: 10.1136/heartjnl-2017-311583
[7] He W, Huang Y, Zhang Y, et al. Cardiac rehabilitation therapy for coronary slow flow phenomenon[J]. Herz, 2020, 45(5): 468-474. doi: 10.1007/s00059-018-4742-y
[8] Caiazzo G, Musci RL, Frediani L, et al. State of the Art: No-Reflow Phenomenon[J]. Cardiol Clin, 2020, 38(4): 563-573. doi: 10.1016/j.ccl.2020.07.001
[9] Keller AC, Klawitter J, Hildreth KL, et al. Elevated plasma homocysteine and cysteine are associated with endothelial dysfunction across menopausal stages in healthy women[J]. J Appl Physiol(1985), 2019, 126(6): 1533-1540. doi: 10.1152/japplphysiol.00819.2018
[10] Li S, Pan G, Chen H, et al. Determination of Serum Homocysteine and Hypersensitive C-reactive Protein and Their Correlation with Premature Coronary Heart Disease[J]. Heart Surg Forum, 2019, 22(3): E215-E217. doi: 10.1532/hsf.2223
[11] 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019(10): 766-783.
[12] Fonseca FA, Izar MC. Role of Inflammation in Cardiac Remodeling After Acute Myocardial Infarction[J]. Front Physiol, 2022, 13: 927163. doi: 10.3389/fphys.2022.927163
[13] Yan J, Zhou J, Huang J, et al. The outcomes of acute myocardial infarction patients comorbidity with hypertension and hyperhomocysteinemia[J]. Sci Rep, 2021, 11(1): 22936. doi: 10.1038/s41598-021-02340-w
[14] Rathod KS, Jones DA, Jain AK, et al. The influence of biological age and sex on long-term outcome after percutaneous coronary intervention for ST-elevation myocardial infarction[J]. Am J Cardiovasc Dis, 2021, 11(5): 659-678.
[15] Kodliwadmath A, Nanda N, Duggal B, et al. Comparative study of acute coronary syndrome in postmenopausal women and age-matched men: A prospective cohort study in Southern India[J]. Ann Afr Med, 2022, 21(1): 8-15. doi: 10.4103/aam.aam_38_20
[16] Nie G, Yang X, Wang Y, et al. The Effects of Menopause Hormone Therapy on Lipid Profile in Postmenopausal Women: A Systematic Review and Meta-Analysis[J]. Front Pharmacol, 2022, 13: 850815. doi: 10.3389/fphar.2022.850815
[17] Kjaergaard AD, Wu Y, Ming WK, et al. Homocysteine and female fertility, pregnancy loss and offspring birthweight: a two-sample Mendelian randomization study[J]. Eur J Clin Nutr, 2022, 76(1): 40-47. doi: 10.1038/s41430-021-00898-2
[18] Pantea-Roşan LR, Pantea VA, Bungau S, et al. No-Reflow after PPCI-A Predictor of Short-Term Outcomes in STEMI Patients[J]. J Clin Med, 2020, 9(9): 2956. doi: 10.3390/jcm9092956
[19] Bossenmeyer-Pourié C, Smith AD, Lehmann S, et al. N-homocysteinylation of tau and MAP1 is increased in autopsy specimens of Alzheimer's disease and vascular dementia[J]. J Pathol, 2019, 248(3): 291-303. doi: 10.1002/path.5254
[20] Chu S, Mao XD, Wang L, et al. Effects of Huang Qi Decoction on Endothelial Dysfunction Induced by Homocysteine[J]. Evid Based Complement Alternat Med, 2016: 7272694.
[21] 马娟, 严宁, 马学平, 等. Hcy联合CRP/Alb比值对STEMI合并代谢综合征患者急诊PCI术后无复流的预测价值[J]. 临床心血管病杂志, 2022, 38(4): 308-314. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202204011.htm
[22] Wagdy S, Sobhy M, Loutfi M. Neutrophil/lymphocyte ratio as a predictor of in-hospital major adverse cardiac events, new-onset atrial fibrillation, and no-reflow phenomenon in patients with ST elevation myocardial infarction[J]. Clin Med Insights Cardiol, 2016, 10(10): 19-22.
[23] Del Turco S, Basta G, De Caterina AR, et al. Different inflammatory profile in young and elderly STEMI patients undergoing primary percutaneous coronary intervention(PPCI): Its influence on no-reflow and mortality[J]. Int J Cardiol, 2019, 290: 34-39. doi: 10.1016/j.ijcard.2019.05.002
[24] Khan KA, Qamar N, Saghir T, et al. Comparison of Intracoronary Epinephrine and Adenosine for No-Reflow in Normotensive Patients With Acute Coronary Syndrome(COAR Trial)[J]. Circ Cardiovasc Interv, 2022, 15(2): e011408. doi: 10.1161/CIRCINTERVENTIONS.121.011408
[25] van Leeuwen M, van der Hoeven NW, Janssens GN, et al. Evaluation of Microvascular Injury in Revascularized Patients With ST-Segment-Elevation Myocardial Infarction Treated With Ticagrelor Versus Prasugrel[J]. Circulation, 2019, 139(5): 636-646. doi: 10.1161/CIRCULATIONAHA.118.035931
[26] Hausenloy DJ, Kharbanda RK, Møller UK, et al. Effect of remote ischaemic conditioning on clinical outcomes in patients with acute myocardial infarction(CONDI-2/ERIC-PPCI): a single-blind randomised controlled trial[J]. Lancet, 2019, 394(10207): 1415-1424. doi: 10.1016/S0140-6736(19)32039-2
[27] Ma M, Wang L, Diao KY, et al. A randomized controlled clinical trial of prolonged balloon inflation during stent deployment strategy in primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: a pilot study[J]. BMC Cardiovasc Disord, 2022, 22(1): 30. doi: 10.1186/s12872-022-02477-0
[28] David SW, Khan ZA, Patel NC, et al. Evaluation of intracoronary hyperoxemic oxygen therapy in acute anterior myocardial infarction: The IC-HOT study[J]. Catheter Cardiovasc Interv, 2019, 93(5): 882-890. doi: 10.1002/ccd.27905
-
图(1)
表(5)
计量
- 文章访问数: 380
- PDF下载数: 79
- 施引文献: 0