
The efficacy of circumferential pulmonary vein combined with additional ablation in reducing recurrence of atrial fibrillation after radiofrequency ablation: a meta-analysis
-
摘要: 目的 探究相比于单纯环肺静脉消融(CPVI),CPVI联合额外部位消融(包括二尖瓣环峡部、三尖瓣环峡部、上腔静脉、左心房顶部、左心房后壁、Marshall静脉、复杂碎裂电位、神经节)是否降低消融术后房颤(AF)的复发率。方法 计算机检索中国知网、万方、维普、中国生物医学文献数据库、PubMed、Embase、Cochrane Library等数据库,筛选出近10年符合标准的随机对照研究,应用Stata软件进行meta分析,比较单纯CPVI与CPVI联合额外部位消融策略在消融后AF复发中的差异。结果 共纳入21篇文献。meta分析结果表明,与单纯CPVI相比,CPVI联合额外部位消融未降低AF复发率。根据额外消融部位、AF类型、左心房内径、AF持续时间进行亚组分析,发现只在较小的左心房内径亚组中,CPVI联合额外部位消融进一步降低AF的复发率(OR=0.68,95%CI:0.47~0.98,P=0.040),在其他亚组中未发现上述现象。结论 相比于单纯CPVI,CPVI联合额外部位的消融策略未降低消融后AF的复发率。Abstract: Objective To investigate whether circumferential pulmonary vein isolation(CPVI) combined with additional ablation(mitral isthmus, tricuspid isthmus, superior vena cava, left atrial roof, left atrial posterior wall, the vein of marshall, complex fractionated atrial electrograms, ganglionated plexi) reduces the recurrence rate of atrial fibrillation(AF) compared with CPVI alone.Methods A literature search was conducted using the databases CNKI, WanFang, VIP, CBM, PubMed, Embase, Cochrane Library. Randomized controlled studies that met the standards in the past ten years were screened out, and the relevant literature contents were meta-analyzed by Stata software. The content about comparing CPVI alone with CPVI combined with the additional ablation strategies in the recurrence of AF was summarized.Results A total of 21 papers were included. Meta-analysis showed that no significant difference between CPVI alone and CPVI combined ablation strategies in reducing AF recurrence. Subgroup analysis based on additional ablation site, AF type, left atrial diameter, AF diagnosis time, and outcome indicators showed that only in the small left atrial diameter subgroup, CPVI combined with additional ablation further reduced the recurrence rate of AF(OR=0.68, 95%CI: 0.47-0.98, P=0.040), which was not found in other subgroups.Conclusion The ablation strategy of CPVI combined with additional sites does not reduce the recurrence rate of AF compared with CPVI alone.
-

-
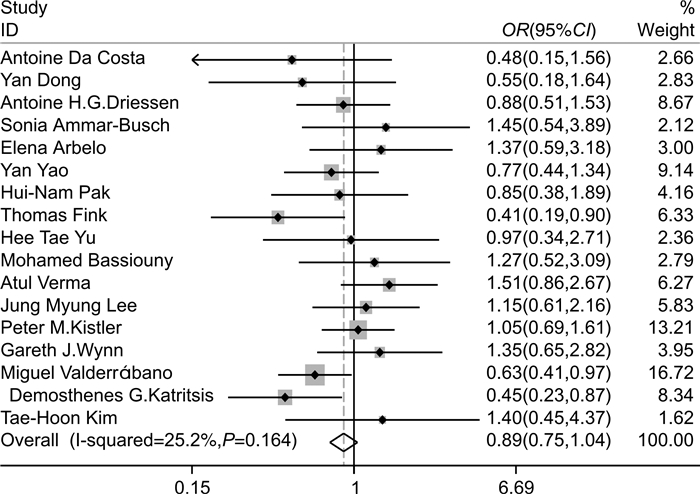
图 2 CPVI联合额外部位与单纯CPVI消融复发率的森林图
Figure 2. The forest plot of the recurrence rate of CPVI combined with ablation and CPVI alone
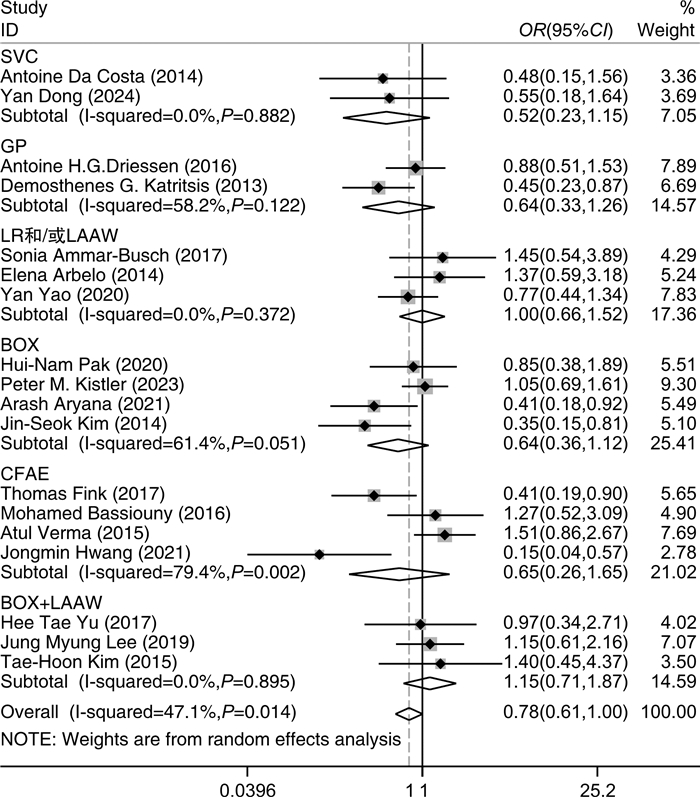
图 3 根据消融部位分析CPVI联合额外部位消融复发率的森林图
Figure 3. The forest plot of the recurrence rate of CPVI combined with different ablation sites
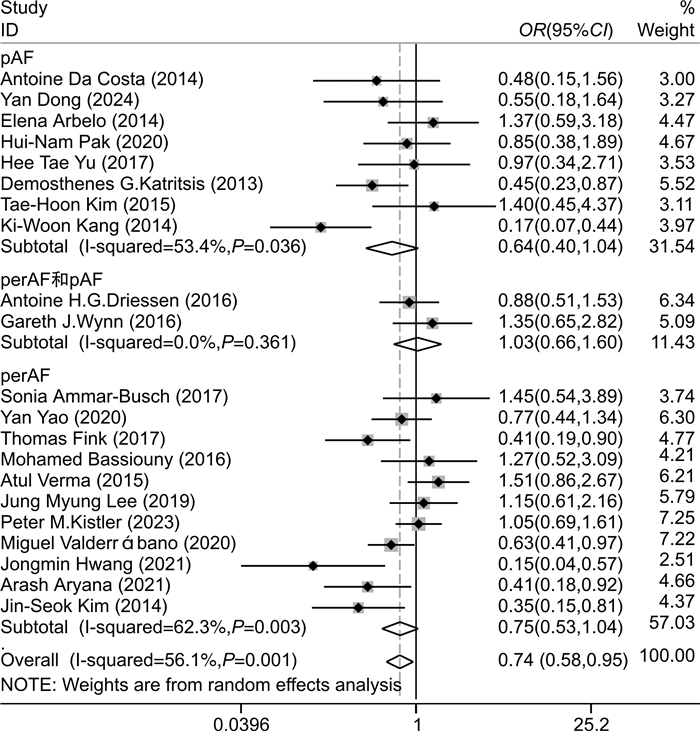
图 4 根据AF类型分析CPVI联合额外部位消融复发率的森林图
Figure 4. The forest plot of the recurrence rate of CPVI combined with ablation according to AF type
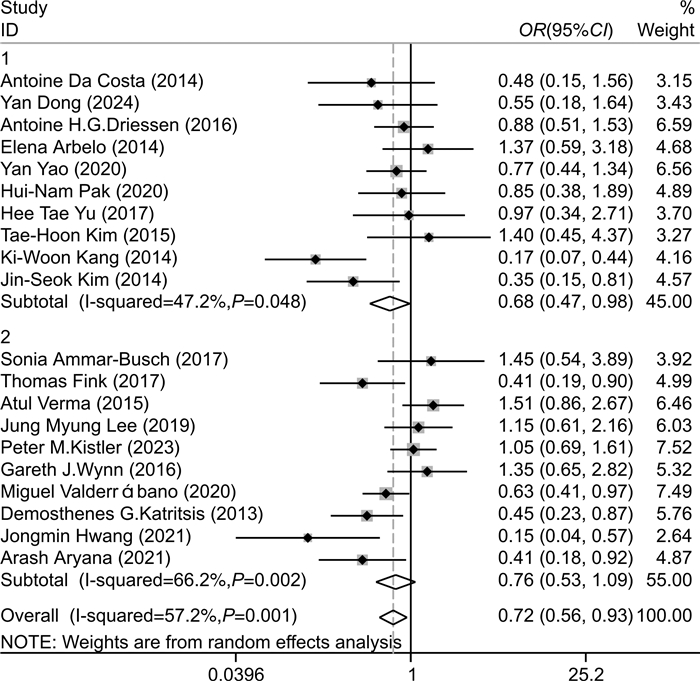
图 5 根据LAD分析CPVI联合额外部位消融复发率的森林图
Figure 5. The forest plot of the recurrence rate CPVI combined with ablation according to LAD
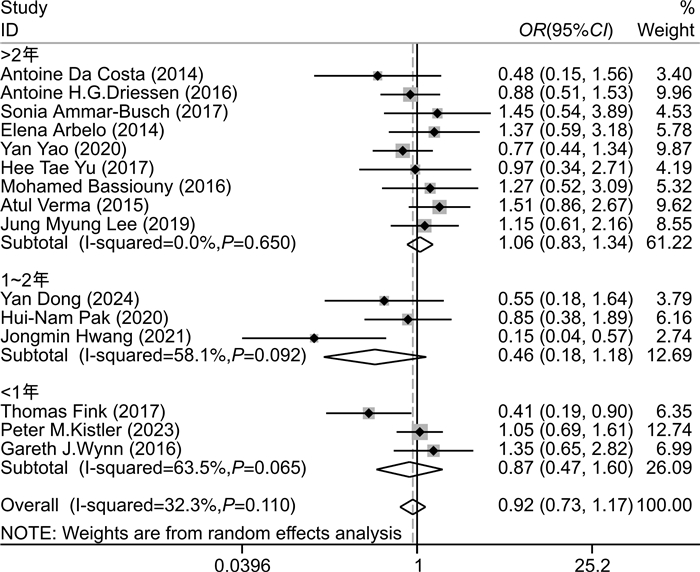
图 6 根据 AF 持续时间分析 CPVI 联合额外部位消融复发率的森林图
Figure 6. The forest plot of the recurrence rate CPVI combined with ablation according to AF duration
表 1 纳入研究的基线特征
Table 1. General characteristics of included studies
X±S, M(P25, P75) 第1作者
(发表年份)研究
类型额外消融
部位AF类型 年龄/岁 男性/% LAD/mm AF持续时间/月 随访时
间/月Jadad
评分对照组 试验组 对照组 试验组 对照组 试验组 对照组 试验组 Da Costa
(2014)[3]随机
双盲SVC pAF 58.0±
9.055.0±
10.079.6 78.4 39.0±
6.042.0±
7.050±
4447.5±
3015±
83 Dong
(2024)[4]随机
非盲SVC pAF 57.1±
9.959.1±
8.974.0 70.0 37.4±
2.938.3±
4.324
(6,72)24
(11,60)12 3 Driessen
(2016)[5]随机
非盲GP perAF和
pAF60.2±
8.259.5±
8.274.0 72.0 42.3±
5.542.1±
5.660
(24,120)48
(24,72)12 4 Ammar-
Busch
(2017)[6]随机
非盲LR+
LAAWperAF 65.0±
8.064.0±
9.082.0 76.0 48.0±
6.049.0±
7.039±
4443±
4812 3 Arbelo
(2014)[7]随机
非盲LR pAF 55.0±
12.055.0±
11.068.9 71.2 41.0±
6.041.0±
6.060±
5659±
5915±
103 Yao(2020)[8] 随机
非盲LAAW perAF 58.0±
9.556.6±
10.780.8 83.7 42.6±
4.541.8±
4.552.7±
5.155.3±
5.424 4 Pak(2020)[9] 随机
单盲BOX pAF 61.6±
7.858.6±
11.470.2 73.7 42.7±
6.141.4±
6.121
(9,71)24
(12,60)23.8±
10.24 Fink
(2017)[10]随机
非盲CFAE perAF 62.1±
9.960.9±
9.669.0 74.0 47.3±
4.546.7±
4.312
(7,24)12
(7,24)12 3 Hwang
(2021)[11]随机
非盲CFAE perAF 57.9±
9.858.8±
9.392.0 80.0 50.0±
6.049.0±
4.027.1±
19.221.4±
26.224.0±
23.14 Yu(2017)[12] 随机
非盲BOX+
LAAWpAF 61.4±
11.159.3±
8.975.0 76.0 42.6±
5.342.7±
5.743.7±
50.841.7±
36.718.6±
11.43 Bassiouny
(2016)[13]随机
非盲CFAE perAF 62.2±
9.464.6±
9.474.0 75.0 45.0±
8.842.0±
9.837
(16,92)45
(17,81)12 4 Verma
(2015)[14]随机
单盲CFAE perAF 58.0±
10.060.0±
9.078.0 81.0 44.0±
6.044.0±
6.051.6±
75.650.4±
6018 5 Lee(2019)[15] 随机
双盲BOX+
LAAWperAF 58.6±
11.058.9±
10.580.0 86.3 44.5±
6.745.0±
5.333.1±
31.444.0±
44.616.2±
8.86 Kistler
(2023)[16]随机
单盲BOX perAF 65.5
(57.8,
71.7)65.7
(58.7,
71.1)76.2 77.1 44.0±
7.046.0±
6.05(2,8) 5(2,8) 12 5 Wynn
(2016)[17]随机
双盲LR+MI+
TIperAF和
pAF61.8±
9.761.9±
11.473.0 62.0 43.0±
6.043.0±
6.05.5±
4.25.5±
3.912 5 Kang
(2014)[18]随机
非盲SVC pAF 55.65±
11.8757.89±
11.4674.0 75.0 39.5±
6.240.1±
5.7- - 12.2±
5.33 Valderrábano
(2020)[19]随机
单盲VOM perAF 66.4±
9.966.6±9.6 78.0 74.0 47.0±
7.544.8±
7.9- - 12 6 Katritsis
(2013)[20]随机
单盲GP pAF 56.0±
7.656.0±
8.568.0 70.0 48.0±
7.048.0±
6.0- - 24 5 Aryana
(2021)[21]随机
双盲BOX perAF 70.0±
9.067.0±
8.060.0 64.0 44.0±
5.044.0±
4.0- - 12 5 Kim
(2014)[22]随机
非盲BOX perAF 58.3±
9.656.2±
11.968.3 76.7 42.1±
5.142.3±
6.4- - 12 4 Kim
(2015)[23]随机
非盲BOX+
LAAWpAF 55.32±
12.4257.72±
10.2280.0 70.0 39.1±
5.941.0±
6.8- - 16.34±
4.004 LAAW:左心房前壁线性消融;BOX:后壁盒式消融;pAF:阵发性房颤;perAF:持续性房颤;-:原文未提供相关数据。  下载: 导出CSV
下载: 导出CSV
表 2 纳入临床研究的研究结果
Table 2. Findings included in clinical studies
例 第1作者(发表年
份)对照组 试验组 RR 复发 总例数 复发 总例数 Costa(2014)[3] 9 49 5 51 0.53 Dong(2024)[4] 10 50 6 50 0.60 Driessen(2016)[5] 39 123 34 117 0.92 Ammar-Busch
(2017)[6]9 45 12 45 1.33 Arbelo(2014)[7] 13 61 16 59 1.27 Yao(2020)[8] 45 105 38 104 0.85 Pak(2020)[9] 18 57 16 57 0.89 Fink(2017)[10] 27 61 14 57 0.55 Hwang(2021)[11] 14 25 4 25 0.29 Yu(2017)[12] 9 59 8 54 0.97 Bassiouny
(2016)[13]30 46 31 44 1.08 Verma(2015)[14] 25 61 125 244 1.25 Lee(2019)[15] 25 105 27 102 1.11 Kistler(2023)[16] 78 168 81 170 1.03 Wynn(2016)[17] 19 64 24 66 1.22 Kang(2014)[18] 27 100 6 100 0.22 Valderrábano
(2020)[19]98 158 94 185 0.82 Katritsis(2013)[20] 34 78 21 82 0.59 Aryana(2021)[21] 25 55 14 55 0.56 Kim(2014)[22] 22 60 10 60 0.45 Kim(2015)[23] 6 50 8 50 1.33
下载: 导出CSV
-
[1] 马长生, 郭雪原. 心房颤动导管消融: 挑战与展望[J]. 临床心血管病杂志, 2015, 31(4): 377-379. doi: 10.13201/j.issn.1001-1439.2015.04.009
[2] Erhard N, Metzner A, Fink T. Late arrhythmia recurrence after atrial fibrillation ablation: incidence, mechanisms and clinical implications[J]. Herzschrittmacherther Elektrophysiol, 2022, 33(1): 71-76. doi: 10.1007/s00399-021-00836-6
[3] Da Costa A, Levallois M, Romeyer-Bouchard C, et al. Remote-controlled magnetic pulmonary vein isolation combined with superior vena cava isolation for paroxysmal atrial fibrillation: a prospective randomized study[J]. Arch Cardiovasc Dis, 2015, 108: 163-171. doi: 10.1016/j.acvd.2014.10.005
[4] Dong Y, Zhao D, Chen X, et al. Role of electroanatomical mapping-guided superior vena cava isolation in paroxysmal atrial fibrillation patients without provoked superior vena cava triggers: a randomized controlled study[J]. Europace, 2024, 26: euae039. doi: 10.1093/europace/euae039
[5] Driessen AHG, Berger WR, Krul SPJ, et al. Ganglion plexus ablation in advanced atrial fibrillation: the AFACT study[J]. J Am Coll Cardiol, 2016, 68: 1155-1165. doi: 10.1016/j.jacc.2016.06.036
[6] Ammar-Busch S, Bourier F, Reents T, et al. Ablation of complex fractionated electrograms with or without additional LINEar lesions for persistent atrial fibrillation(The ADLINE Trial)[J]. J Cardiovasc Electrophysiol, 2017, 28: 636-641. doi: 10.1111/jce.13206
[7] Arbelo E, Guiu E, Ramos P, et al. Benefit of left atrial roof linear ablation in paroxysmal atrial fibrillation: a prospective, randomized study[J]. J Am Heart Assoc, 2014, 3: e000877. doi: 10.1161/JAHA.114.000877
[8] Yao Y, Hu F, Du Z, et al. The value of extensive catheter linear ablation on persistent atrial fibrillation(the CLEAR-AF Study)[J]. Int J Cardiol, 2020, 316: 125-129. doi: 10.1016/j.ijcard.2020.05.032
[9] Pak HN, Park J, Park JW, et al. Electrical posterior box isolation in persistent atrial fibrillation changed to paroxysmal atrial fibrillation: a multicenter, prospective, randomized study[J]. Circ Arrhythm Electrophysiol, 2020, 13: e008531. doi: 10.1161/CIRCEP.120.008531
[10] Fink T, Schlüter M, Heeger CH, et al. Stand-alone pulmonary vein isolation versus pulmonary vein isolation with additional substrate modification as index ablation procedures in patients with persistent and long-standing persistent atrial fibrillation: the randomized alster-lost-af trial(ablation at st. georg hospital for long-standing persistent atrial fibrillation)[J]. Circ Arrhythm Electrophysiol, 2017, 10: e005114. doi: 10.1161/CIRCEP.117.005114
[11] Hwang J, Park HS, Han S, et al. Ablation of persistent atrial fibrillation based on high density voltage mapping and complex fractionated atrial electrograms: A randomized controlled trial[J]. Medicine(Baltimore), 2021, 100: e26702.
[12] Yu HT, Shim J, Park J, et al. Pulmonary vein isolation alone versus additional linear ablation in patients with persistent atrial fibrillation converted to paroxysmal type with antiarrhythmic drug therapy: a multicenter, prospective, randomized study[J]. Circ Arrhythm Electrophysiol, 2017, 10: e004915. doi: 10.1161/CIRCEP.116.004915
[13] Bassiouny M, Saliba W, Hussein A, et al. Randomized study of persistent atrial fibrillation ablation: ablate in sinus rhythm versus ablate complex-fractionated atrial electrograms in atrial fibrillation[J]. Circ Arrhythm Electrophysiol, 2016, 9: e003596.
[14] Verma A, Jiang C, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation[J]. N Engl J Med, 2015, 372: 1812-1822. doi: 10.1056/NEJMoa1408288
[15] Lee JM, Shim J, Park J, et al. The electrical isolation of the left atrial posterior wall in catheter ablation of persistent atrial fibrillation[J]. JACC Clin Electrophysiol, 2019, 5: 1253-1261. doi: 10.1016/j.jacep.2019.08.021
[16] Kistler PM, Chieng D, Sugumar H, et al. Effect of catheter ablation using pulmonary vein isolation with vs without posterior left atrial wall isolation on atrial arrhythmia recurrence in patients with persistent atrial fibrillation: the capla randomized clinical trial[J]. JAMA, 2023, 329: 127-135. doi: 10.1001/jama.2022.23722
[17] Wynn GJ, Panikker S, Morgan M, et al. Biatrial linear ablation in sustained nonpermanent AF: Results of the substrate modification with ablation and antiarrhythmic drugs in nonpermanent atrial fibrillation(SMAN-PAF)trial[J]. Heart Rhythm, 2016, 13: 399-406. doi: 10.1016/j.hrthm.2015.10.006
[18] Kang KW, Pak HN, Park J, et al. Additional linear ablation from the superior vena cava to right atrial septum after pulmonary vein isolation improves the clinical outcome in patients with paroxysmal atrial fibrillation: prospective randomized study[J]. Europace, 2014, 16: 1738-1745. doi: 10.1093/europace/euu226
[19] Valderrábano M, Peterson LE, Swarup V, et al. Effect of catheter ablation with vein of marshall ethanol infusion vs catheter ablation alone on persistent atrial fibrillation: The VENUS randomized clinical trial[J]. JAMA, 2020, 324: 1620-1628. doi: 10.1001/jama.2020.16195
[20] Katritsis DG, Pokushalov E, Romanov A, et al. Autonomic denervation added to pulmonary vein isolation for paroxysmal atrial fibrillation: a randomized clinical trial[J]. J Am Coll Cardiol, 2013, 62: 2318-2325. doi: 10.1016/j.jacc.2013.06.053
[21] Aryana A, Allen SL, Pujara DK, et al. Concomitant pulmonary vein and posterior wall isolation using cryoballoon with adjunct radiofrequency in persistent atrial fibrillation[J]. JACC Clin Electrophysiol, 2021, 7: 187-196. doi: 10.1016/j.jacep.2020.08.016
[22] Kim JS, Shin SY, Na JO, et al. Does isolation of the left atrial posterior wall improve clinical outcomes after radiofrequency catheter ablation for persistent atrial fibrillation?A prospective randomized clinical trial[J]. Int J Cardiol, 2015, 181: 277-283. doi: 10.1016/j.ijcard.2014.12.035
[23] Kim TH, Uhm JS, Kim JY, et al. Does additional electrogram-guided ablation after linear ablation reduce recurrence after catheter ablation for longstanding persistent atrial fibrillation? a prospective randomized study[J]. J Am Heart Assoc, 2017, 6: e004811. doi: 10.1161/JAHA.116.004811
[24] Markides V, Schilling RJ, Ho SY, et al. Characterization of left atrial activation in the intact human heart[J]. Circulation, 2003, 107(5): 733-739. doi: 10.1161/01.CIR.0000048140.31785.02
[25] Roberts-Thomson KC, Stevenson IH, Kistler PM, et al. Anatomically determined functional conduction delay in the posterior left atrium relationship to structural heart disease[J]. J Am Coll Cardiol, 2008, 51(8): 856-862. doi: 10.1016/j.jacc.2007.11.037
[26] McLellan AJA, Prabhu S, Voskoboinik A, et al. Isolation of the posterior left atrium for patients with persistent atrial fibrillation: routine adenosine challenge for dormant posterior left atrial conduction improves long-term outcome[J]. Europace, 2017, 19(12): 1958-1966. doi: 10.1093/europace/euw231
[27] Cluckey A, Perino AC, Yunus FN, et al. Efficacy of ablation lesion sets in addition to pulmonary vein isolation for paroxysmal atrial fibrillation: findings from the SMASH-AF meta-analysis study cohort[J]. J Am Heart Assoc, 2019, 8: e009976. doi: 10.1161/JAHA.118.009976
[28] Hu X, Jiang J, Ma Y, et al. Is there still a role for additional linear ablation in addition to pulmonary vein isolation in patients with paroxysmal atrial fibrillation? An Updated Meta-analysis of randomized controlled trials[J]. Int J Cardiol, 2016, 209: 266-274. doi: 10.1016/j.ijcard.2016.02.076
[29] 杨再鑫, 杨一桢, 石亮, 等. 左心房基质重构在阵发性心房颤动射频消融术后超远期复发中的作用[J]. 临床心血管病杂志, 2024, 40(6): 488-493. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202406012.htm
[30] Mahnkopf C, Badger TJ, Burgon NS, et al. Evaluation of the left atrial substrate in patients with lone atrial fibrillation using delayed-enhanced MRI: implications for disease progression and response to catheter ablation[J]. Heart Rhythm, 2010, 7: 1475-1481. doi: 10.1016/j.hrthm.2010.06.030
-
计量
- 文章访问数: 181
- 施引文献: 0