
The value of whole blood transcriptome mRNA in patients with heart failure with preserved ejection fraction
-
摘要: 目的 利用转录组mRNA测序检测射血分数保留型心力衰竭(heart failure with preserved ejection fraction,HFpEF)患者差异表达基因,寻找辅助诊断HFpEF的新型分子生物标志物。方法 本前瞻性研究选取2021年11月—2022年1月于泰达国际心血管病医院治疗的HFpEF患者及同期健康体检者各10例;通过转录组mRNA测序筛选差异表达基因并进行功能富集分析。同时选取2021年11月—2022年12月于泰达国际心血管病医院治疗的HFpEF患者62例(HFpEF组);收集同期健康体检者57例组成健康对照组。实时荧光定量PCR(real-time quantitative PCR,RT-qPCR)检测差异基因在两组中的表达情况。Logistic回归进行差异基因与HFpEF的归因分析。ROC曲线评估差异mRNA的辅助诊断价值。结果 HFpEF组相对于健康对照组共筛选出差异表达基因15个(12个上调基因和3个下调基因)。差异基因富集分析发现关于酮体合成通路和类固醇合成通路上调,过氧化物酶体部分通路下调。选取与心血管疾病发生发展相关的基因KRT1、CA1、GSTM1、SELENBP1、MYOM2、EGR1进行临床人群验证,RT-qPCR结果显示,KRT1、CA1、SELENBP1、EGR1在HFpEF组表达水平显著上调(PKRT1 < 0.001、PCA1=0.029、PSELENBP1 < 0.001、PEGR1=0.005),MYOM2显著下调(PMYOM2=0.006)。多因素logistic回归分析显示KRT1、CA1是HFpEF的独立预测因子。KRT1、CA1及二者联合的辅助诊断价值AUC分别为0.717(P < 0.001)、0.610(P=0.039)、0.801(P < 0.001)。结论 转录组mRNA测序分析筛选了HFpEF相对健康对照组的差异表达基因,KRT1联合CA1可作为辅助诊断HFpEF的新型分子生物标志物;富集结果提示HFpEF的发病机制可能与脂类代谢、类固醇激素合成以及氧化应激有关。
-
关键词:
- 射血分数保留型心力衰竭 /
- 转录组mRNA /
- 新型生物标志物
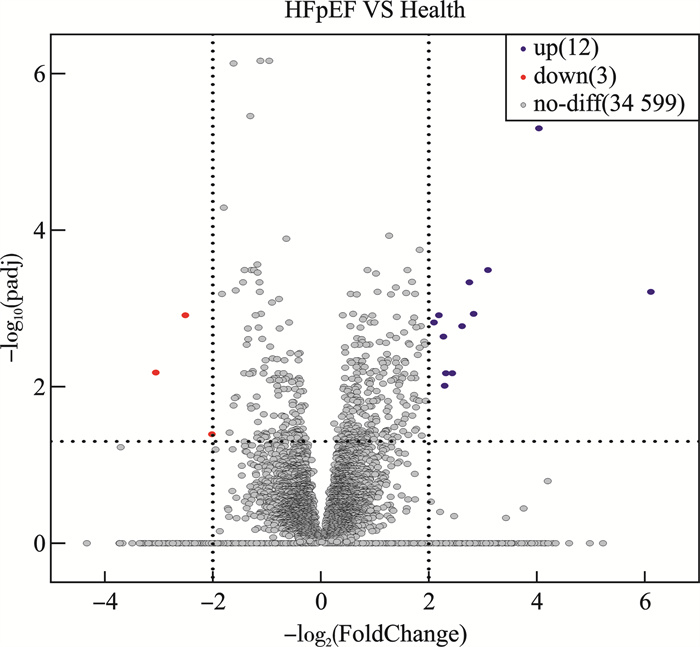
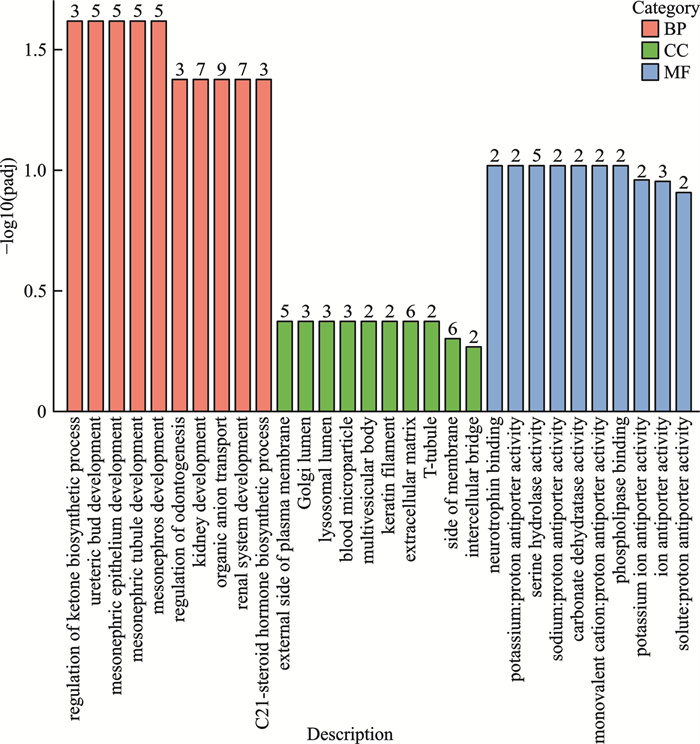
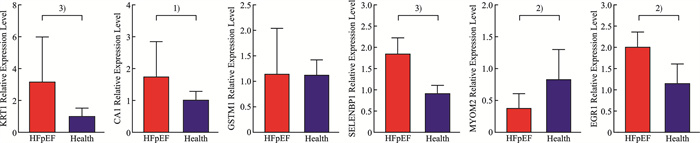
Abstract: Objective Transcriptome mRNA sequencing was used to detect the differentially expressed genes in patients with heart failure with preserved ejection fraction(HFpEF) to search for novel molecular biomarkers to aid in the diagnosis of HFpEF.Methods For the prospective study, 10 patients with HFpEF treated at Teda International Cardiovascular Disease Hospital from November 2021 to January 2022 and 10 patients with health checkups during the same period were selected. Differentially expressed genes were screened by transcriptome mRNA sequencing and analysed for functional enrichment. 62 patients with HFpEF treated at TEDA International Cardiovascular Hospital from November 2021 to December 2022 were selected, and 57 cases were selected from the same period of health checks to form a healthy controls. Real-time quantitative PCR(RT-qPCR) was used to detect the expression of differential genes in the two groups. Logistic regression was used to analyse the attribution of differential genes to HFpEF. ROC curves to evaluate the adjunctive diagnostic value of differential mRNA.Results A total of 15 differentially expressed genes(12 upregulated and 3 downregulated genes) were screened in the HFpEF compared to healthy controls. Differential gene enrichment analyses revealed upregulation of the ketone biosynthesis pathway and the steroid hormone biosynthesis pathway, and downregulation of peroxisomal part pathway. The genes KRT1, CA1, GSTM1, SELENBP1, MYOM2, and EGR1, which are associated with the development of cardiovascular disease, were selected for validation in clinical populations. RT-qPCR results showed that the expression levels of KRT1, CA1, SELENBP1 and EGR1 were significantly upregulated in HFpEF group(PKRT1 < 0.001、PCA1=0.029、PSELENBP1 < 0.001、PEGR1=0.005), and MYOM2 was significantly downregulated(PMYOM2=0.006). Logistic regression analysis showed that KRT1 and CA1 were independent predictors of HFpEF. The AUC for the adjunctive diagnostic value of KRT1, CA1 and their combination were 0.717(P < 0.001), 0.610(P=0.039) and 0.801(P < 0.001).Conclusion Transcriptome mRNA sequencing analysis screened for differentially expressed genes in HFpEF compared to healthy controls, and KRT1 combined with CA1 can be used as a novel molecular biomarker to help diagnose HFpEF. The enrichment results suggest that the pathogenesis of HFpEF may be related to lipid metabolism, steroid hormone synthesis and oxidative stress. -

-

图 2 HFpEF组与健康对照组差异表达基因聚类热图
Figure 2. Cluster heatmap of differentially expressed genes
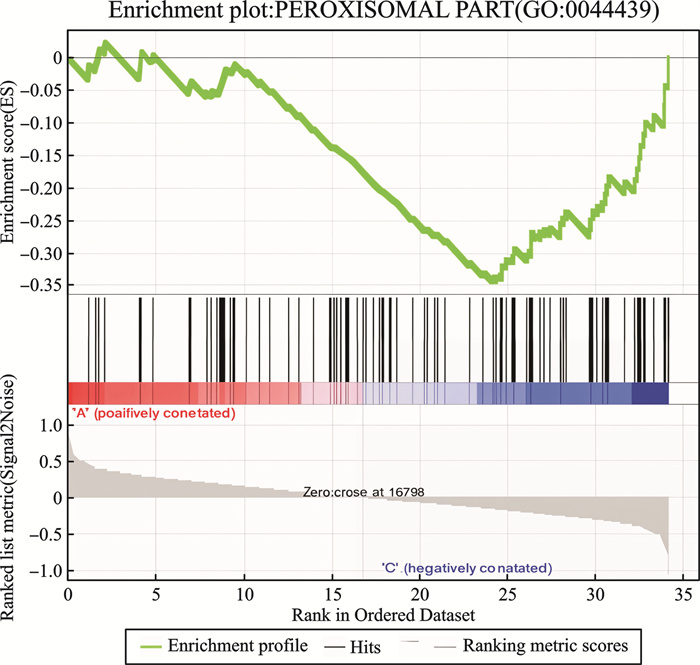
图 4 GSEA富集图:过氧化物酶体部分(GO:0044439)
Figure 4. GSEA enrichment map: Peroxisome portion(GO: 0044439)

图 6 KRT1、CA1及二者联合辅助诊断HFpEF的ROC曲线分析
Figure 6. ROC of KRT1, CA1 and their combined auxiliary diagnosis of HFpEF
表 1 HFpEF组和健康对照组差异表达基因
Table 1. Differential expression genes between HFpEF and healthy control group
基因缩写 基因描述 log2(FoldChange) Padj 上调差异基因 KRT1 Keratin 1角蛋白1 4.04 < 0.001 CA1 Carbonic Anhydrase 1碳酸酐酶1 3.10 < 0.001 SNCA α-synuclein α-突触核蛋白 2.75 < 0.001 GSTM1 Glutathione S-transferase M 1谷胱甘肽硫转移酶M1 6.11 0.001 ALAS2 5'-aminolevulinate Synthase 2 5'-氨基乙酰丙酸合成酶2 2.83 0.001 SLC4A1 Solute Carrier Family 4 Member 1溶质载体家族4成员1 2.19 0.001 SELENBP1 Selenium-binding Protein 1硒结合蛋白1 2.10 0.002 SLC2A4 Solute Carrier Family 2 Member 4溶质载体家族2成员4 2.62 0.002 GYPB Glycophorin B血型糖蛋白B 2.27 0.002 PAQR9 Progestin and AdipoQ Receptor Family Member 9孕激素和脂联素受体家族成员9 2.43 0.007 BCAM Basal Cell Adhesion Molecule基底细胞黏附分子 2.32 0.007 EGR1 Early Growth Response 1早期生长反应因子1 2.29 0.010 下调差异基因 FOLR3 Folate Receptor 3叶酸受体3 -2.50 0.001 MYOM2 Myomesin 2肌间蛋白2 -3.05 0.007 KIR3DL1 Killer Cell Immunoglobulin-like Receptor,Three Ig Domains and Long Cytoplasmic Tail 1杀伤细胞免疫球蛋白样受体3DL1 -2.01 0.041 注:Padj:多重假设检验校正后的P值。  下载: 导出CSV
下载: 导出CSV
表 2 HFpEF和健康对照组的临床基线资料
Table 2. Clinical baseline data
例(%), M(P25, P75), X±S 参数 HFpEF组(62例) 健康对照组(57例) χ2/Z/t P 男性 20(32.26) 37(64.91) 12.689 < 0.001 年龄/岁 71.00(64.00,76.00) 60.00(58.00,64.00) -5.878 < 0.001 BMI/(kg/m2) 25.11(22.62,27.93) 24.35(22.58,26.57) -1.175 0.240 收缩压/mmHg 135.00(123.00,14.50) 133.00(124.50,138.00) -1.918 0.055 舒张压/mmHg 77.00(67.00,88.50) 79.00(73.00,84.50) -0.369 0.712 高血压 57(91.94) 11(19.30) 63.981 < 0.001 糖尿病 28(45.16) 5(8.77) 19.622 < 0.001 LVEF/% 57.73±4.71 62.55±2.56 -4.366 < 0.001 LVMI/(g/m2) 116.06(105.22,131.19) 86.35(80.36,91.56) -6.575 < 0.001 CREA/(μmol/L) 63.00(53.75,81.25) 65.00(55.50,81.25) -0.53 0.596 eGFR/(mL/min/1.73 m2) 90.23(65.19,107.39) 106.05(93.02,125.22) -4.045 < 0.001 UA/(μmol/L) 290.50(233.50,372.25) 324.00(271.50,376.00) -1.096 0.273 UREA/(mmol/L) 6.30(5.28,7.90) 5.30(4.60,6.65) -2.413 0.016 HDL-C/(mmol/L) 1.05(0.93,1.29) 1.32(1.14,1.57) -4.109 < 0.001 LDL-C/(mmol/L) 2.22(1.74,3.44) 3.03(2.46,3.49) -3.025 0.002 ALT/(U/L) 14.00(11.00,23.50) 17.00(13.00,23.50) -1.605 0.108 TBIL/(μmol/L) 8.70(6.40,12.50) 10.90(7.80,12.75) -1.538 0.124 ALB/(g/L) 39.00(37.00,42.00) 45.00(43.75,46.25) -5.782 < 0.001 BNP(pg/mL) 449.00(267.75,770.25) 24.00(15.00,39.00) -9.283 < 0.001 注:BMI:体重指数;LVMI:左心室质量指数;CREA:肌酐;eGFR:肾小球滤过率;UA:尿酸;UREA:尿素;HDL-C:高密度脂蛋白胆固醇;LDL-C:低密度脂蛋白胆固醇;ALT:丙氨酸氨基转移酶;TBIL:总胆红素;ALB:白蛋白;BNP:B型利钠肽。
下载: 导出CSV
表 3 Logistic回归分析
Table 3. Logistic regression analysis
因素 单因素分析 多因素分析 OR(95%CI) P OR(95%CI) P KRT1 1.086(1.026~1.149) 0.005 1.113(1.037~1.195) 0.003 CAI 1.188(1.017~1.388) 0.030 1.477(1.147~1.903) 0.003 SELENBP1 1.613(1.191~2.186) 0.002 MYOM2 0.772(0.594~1.004) 0.054 EGR1 0.994(0.948~1.042) 0.801
下载: 导出CSV
表 4 KRT1和CA1辅助诊断HFpEF的ROC曲线分析
Table 4. ROC of KRT1 and CA1 assisted diagnosis of HFpEF
检验变量 灵敏度/% 特异度/% P 截断值 AUC 95%CI KRT1 49.2% 82.1% < 0.001 3.266 0.717 0.624~0.809 CA1 45.9% 84.2% 0.039 2.257 0.610 0.506~0.714 KRT1联合CA1 72.4% 82.1% < 0.001 0.801 0.719~0.883
下载: 导出CSV
-
[1] 周京敏, 王华, 黎励文. 射血分数保留的心力衰竭诊断与治疗中国专家共识2023 [J]. 中国循环杂志, 2023, 38(4): 375-393.
[2] Cai AP, Qiu WD, Zhou YL, et al. Clinical characteristics and 1-year outcomes in hospitalized patients with heart failure with preserved ejection fraction: results from the China Cardiovascular Association Database-Heart Failure Center Registry [J]. Eur J Heart Fail, 2022, 24(11): 2048-2062.
[3] 王华, 刘宇佳, 杨杰孚. 心力衰竭流行病学[J]. 临床心血管病杂志, 2023, 39(4): 243-247. doi: 10.13201/j.issn.1001-1439.2023.04.001
[4] McDonagh TA, Metra M, Adamo M, et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [J]. Eur Heart J, 2023, 44(37): 3627-3639.
[5] 中华医学会心血管病学分会, 中国医师协会心血管内科医师分会, 中国医师协会心力衰竭专业委员会, 等. 中国心力衰竭诊断和治疗指南2024 [J]. 中华心血管病杂志, 2024, 52(3): 235-275.
[6] Pieske B, Tschöpe C, de Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association(HFA)of the European Society of Cardiology(ESC) [J]. Eur Heart J, 2019, 40(40): 3297-3317. doi: 10.1093/eurheartj/ehz641
[7] Konstam MA, Abboud FM. Ejection fraction: misunderstood and overrated(changing the paradigm in categorizing heart failure) [J]. Circulation, 2017, 135(8): 717-719. doi: 10.1161/CIRCULATIONAHA.116.025795
[8] Pellikka PA, She LL, Holly TA, et al. Variability in ejection fraction measured by echocardiography, gated single-photon emission computed tomography, and cardiac magnetic resonance in patients with coronary artery disease and left ventricular dysfunction [J]. JAMA Netw Open, 2018, 1(4): e181456. doi: 10.1001/jamanetworkopen.2018.1456
[9] Cannata A, McDonagh TA. Heart failure with preserved ejection fraction [J]. N Engl J Med, 2025, 392(2): 173-184. doi: 10.1056/NEJMcp2305181
[10] Hahn VS, Knutsdottir H, Luo X, et al. Myocardial gene expression signatures in human heart failure with preserved ejection fraction [J]. Circulation, 2021, 143(2): 120-134. doi: 10.1161/CIRCULATIONAHA.120.050498
[11] Ye B, Bradshaw AD, Abrahante JE, et al. Left ventricular gene expression in heart failure with preserved ejection fraction-profibrotic and proinflammatory pathways and genes [J]. Circ Heart Fail, 2023, 16(8): e010395.
[12] Inácio JM, Cristo F, Pinheiro M, et al. Myocardial RNA sequencing reveals new potential therapeutic targets in heart failure with preserved ejection fraction [J]. Biomedicines, 2023, 11(8): 2131. doi: 10.3390/biomedicines11082131
[13] McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [J]. Eur Heart J, 2021, 42(36): 3599-3726. doi: 10.1093/eurheartj/ehab368
[14] Das S, Frisk C, Eriksson MJ, et al. Transcriptomics of cardiac biopsies reveals differences in patients with or without diagnostic parameters for heart failure with preserved ejection fraction [J]. Sci Rep, 2019, 9(1): 3179. doi: 10.1038/s41598-019-39445-2
[15] He S, Zhao L, Zhang JJ, et al. Identification of molecular signatures in epicardial adipose tissue in heart failure with preserved ejection fraction [J]. ESC Heart Fail, 2024, 11(5): 2510-2520. doi: 10.1002/ehf2.14748
[16] Devaux Y. Transcriptome of blood cells as a reservoir of cardiovascular biomarkers [J]. Biochim Biophys Acta Mol Cell Res, 2017, 1864(1): 209-216. doi: 10.1016/j.bbamcr.2016.11.005
[17] Chen F, Yang JF, Li YY, et al. Circulating microRNAs as novel biomarkers for heart failure [J]. Hellenic J Cardiol, 2018, 59(4): 209-214. doi: 10.1016/j.hjc.2017.10.002
[18] Gao ZF, Ji XL, Gu J, et al. microRNA-107 protects against inflammation and endoplasmic reticulum stress of vascular endothelial cells via KRT1-dependent Notch signaling pathway in a mouse model of coronary atherosclerosis [J]. J Cell Physiol, 2019, 234(7): 12029-12041. doi: 10.1002/jcp.27864
[19] 贾义, 代杰, 张亮亮, 等. 硒结合蛋白1的生物功能及其与疾病的关系[J]. 生物化学与生物物理进展, 2019, 46(2): 128-137.
[20] Simeunovic D, Odanovic N, Pljesa-Ercegovac M, et al. Glutathione transferase P1 polymorphism might be a risk determinant in heart failure [J]. Dis Markers, 2019: 6984845.
[21] Song XQ, Song Y, Ma QP, et al. M1-type macrophages secrete TNF-α to stimulate vascular calcification by upregulating CA1 and CA2 expression in VSMCs [J]. J Inflamm Res, 2023, 16: 3019-3032.
[22] Marques FZ, Nelson E, Chu PY, et al. High-fiber diet and acetate supplementation change the gut microbiota and prevent the development of hypertension and heart failure in hypertensive mice [J]. Circulation, 2017, 135(10): 964-977.
[23] Huang K, Wu H, Xu XY, et al. Identification of TGF-β-related genes in cardiac hypertrophy and heart failure based on single cell RNA sequencing [J]. Aging, 2023, 15(14): 7187-7218.
[24] Auxerre-Plantié E, Nielsen T, Grunert M, et al. Identification of MYOM2 as a candidate gene in hypertrophic cardiomyopathy and Tetralogy of Fallot, and its functional evaluation in the Drosophila heart [J]. Dis Model Mech, 2020, 13(12): dmm045377.
[25] Mason JM, Hancock HC, Close H, et al. Utility of biomarkers in the differential diagnosis of heart failure in older people: findings from the heart failure in care homes(HFinCH)diagnostic accuracy study [J]. PLoS One, 2013, 8(1): e53560.
[26] Celik A, Koc F, Kadi H, et al. Relationship between red cell distribution width and echocardiographic parameters in patients with diastolic heart failure [J]. Kaohsiung J Med Sci, 2012, 28(3): 165-172.
[27] Remmelzwaal S, van Ballegooijen AJ, Schoonmade LJ, et al. Natriuretic peptides for the detection of diastolic dysfunction and heart failure with preserved ejection fraction-a systematic review and meta-analysis [J]. BMC Med, 2020, 18(1): 290.
[28] Wang R, Capone F, Capone F, et al. Ketone-based metabolism and signalling in heart failure with preserved ejection fraction(HFpEF) [J]. Cardiovasc Res, 2024, 120(Supplement_1): cvae088.096.
[29] Deng Y, Xie MD, Li Q, et al. Targeting mitochondria-inflammation circuit by β-hydroxybutyrate mitigates HFpEF [J]. Circ Res, 2021, 128(2): 232-245.
[30] Sun QY, Güven B, Wagg CS, et al. Mitochondrial fatty acid oxidation is the major source of cardiac adenosine triphosphate production in heart failure with preserved ejection fraction [J]. Cardiovasc Res, 2024, 120(4): 360-371.
[31] Li JX, Cummins CL. Fresh insights into glucocorticoid-induced diabetes mellitus and new therapeutic directions [J]. Nat Rev Endocrinol, 2022, 18(9): 540-557.
[32] Jia GH, Lockette W, Sowers JR. Mineralocorticoid receptors in the pathogenesis of insulin resistance and related disorders: from basic studies to clinical disease [J]. Am J Physiol Regul Integr Comp Physiol, 2021, 320(3): R276-R286.
[33] She PL, Gao BJ, Li DL, et al. The transcriptional repressor HEY2 regulates mitochondrial oxidative respiration to maintain cardiac homeostasis [J]. Nat Commun, 2025, 16(1): 232.
[34] Lanzer JD, Valdeolivas A, Pepin M, et al. A network medicine approach to study comorbidities in heart failure with preserved ejection fraction [J]. BMC Med, 2023, 21(1): 267.
-
计量
- 文章访问数: 222
- 施引文献: 0