
Evaluation value of intravascular ultrasound signs for non-target vessel restenosis 1 year after PCI in patients with coronary heart disease
-
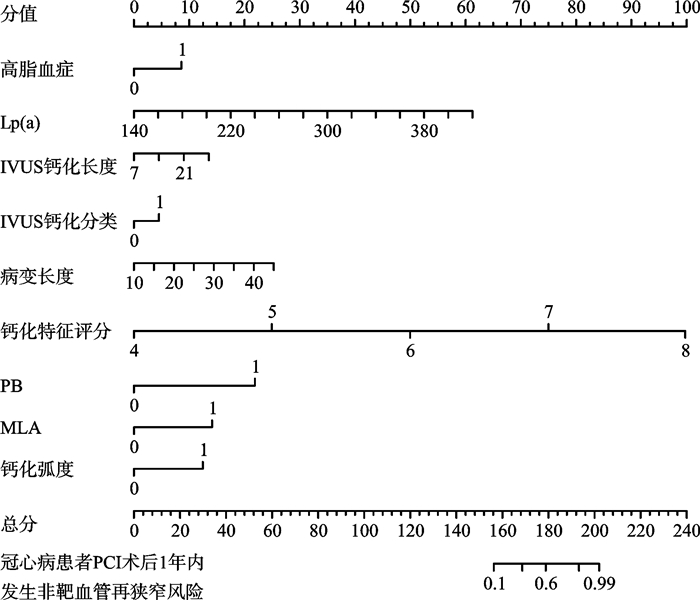
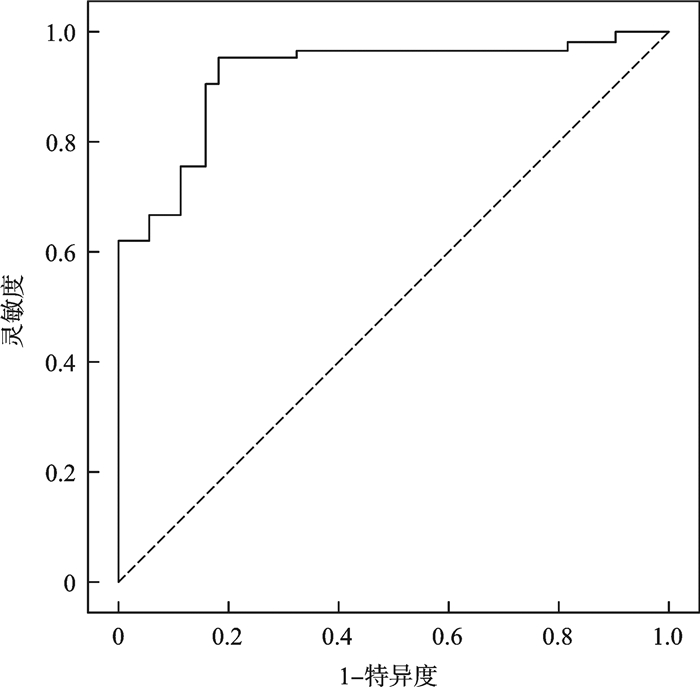
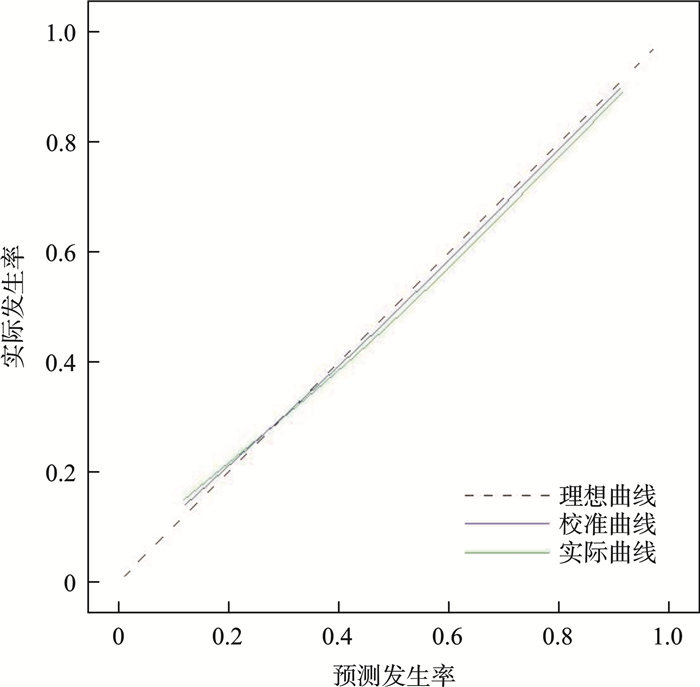
摘要: 目的 探究血管内超声(IVUS)征象对冠心病患者经皮冠状动脉介入(PCI)术后1年出现非靶血管再狭窄的评估价值。方法 纳入2020年12月—2023年7月在本院接受PCI术治疗的90例冠心病患者。随访1年,期间2例患者分别因恶性肿瘤和严重感染死亡,最终纳入88例。根据PCI术后1年是否发生非靶血管再狭窄,将所纳入患者分为再狭窄组(21例)和非再狭窄组(67例)。于PCI术前对患者进行IVUS检查,筛选发生非靶血管再狭窄的危险因素,构建风险预测模型,并进行验证。结果 高脂血症、脂蛋白a[Lp(a)]、IVUS钙化长度、浅层/混合钙化、病变长度、钙化特征评分斑块负荷(PB)>70%、最小管腔面积(MLA)≤4 mm2、钙化弧度(91°~360°)均是冠心病患者PCI术后1年内发生非靶血管再狭窄的危险因素(均P<0.05)。列线图风险模型预测冠心病患者PCI术后1年内发生非靶血管再狭窄的ROC曲线下面积(AUC)、灵敏度、特异度分别为0.881(95%CI:0.618~0.994)、95.70%、77.60%(P<0.001)。Bootstrap法检测C指数为0.842(95%CI:0.768~0.987)。预测值与实际预测值均在理想曲线附近,且Hosmer-Lemeshow拟合优度曲线检验χ2=1.736、P=0.721。结论 基于IVUS征象结合其他危险因素构建的预测模型对冠心病PCI术后1年内发生非靶血管再狭窄具有较高的预测价值,且校准度、拟合优度较好,可为临床预后判断提供理论指导。Abstract: Objective To evaluate the value of intravascular ultrasound (IVUS) features for non-target vessel restenosis one year after percutaneous coronary intervention (PCI) in patients with coronary heart disease.Methods A total of 90 patients with coronary heart disease who underwent at our hospital from December 2020 to July 2023 were enrolled. During the one-year follow-up period, two patients died due to malignancy and severe infection, respectively, resulting in a final inclusion of 88 patients. Based on the occurrence of non-target vessel restenosis within one year after PC, patients were divided into the restenosis group (n=21) and the non-restenosis group (n=67). IVUS was performed prior to PCI to identify features associated with non-target vessel restenosis. Risk factors were analyzed to construct and validate a risk prediction model.Results Hyperlipidemia, Lp(a), IVUS calcification length, shallow/mixed calcification, lesion length, calcification feature score plaque burden (PB) > 70%, minimal luminal area (MLA)≤4 mm2, and calcification arc (91°~360°) were all identified as risk factors for non-target vessel restenosis in coronary heart disease patients within 1 year after PCI (all P<0.05). The nomogram-based risk model prediction model demonstrated an area under the ROC curve (AUC) of 0.881 (95%CI: 0.618-0.994), sensitivity of 95.70%, specificity of 77.60% (P<0.001). The C index detected by Bootstrap method was 0.842 (95%CI: 0.768-0.987). The predicted values closely matched the actual outcomes, and the Hosmer-Lemeshow goodness-of-fit curve test showed χ2=1.736, P=0.721.Conclusion The predictive model based on IVUS signs combined with clinical risk factors demonstrates high accuracy and good calibration for predicting non-target vessel restenosis within one year after PCI in patients with coronary heart disease. This model offers valuable theoretical guidance for clinical management.
-

-
表 1 非再狭窄组和再狭窄组患者临床资料
Table 1. Clinical data in the non-restenosis group and the restenosis group
例(%), X±S 项目 非再狭窄组(67例) 再狭窄组(21例) χ2/t P 性别 0.177 0.674 男 38(56.72) 13(61.90) 女 29(43.28) 8(38.10) 年龄/岁 64.81±9.25 65.23±8.87 0.171 0.865 BMI/(kg/m2) 23.37±1.41 23.42±1.32 0.134 0.894 合并基础病 糖尿病 9(13.43) 4(19.05) 0.400 0.527 高血压 11(16.42) 4(19.05) 0.078 0.780 高脂血症 10(14.93) 9(42.86) 7.368 0.007 吸烟史 12(17.91) 3(14.29) 0.149 0.700 饮酒史 9(13.43) 4(19.05) 0.400 0.527 病变血管支数 1.387 0.500 单支 32(47.76) 7(33.33) 双支 21(31.34) 8(38.10) 3支 14(20.90) 6(28.57) LVEF/% 54.18±5.78 56.42±6.23 1.400 0.167 支架数量 0.374 0.541 ≤2个 43(64.18) 15(71.43) >2个 24(35.82) 6(28.57) 支架长度 0.727 0.394 ≤20 mm 39(58.21) 10(47.62) >20 mm 28(41.79) 11(52.38) 支架直径/mm 3.02±0.64 2.91±0.55 0.668 0.507 术后规律服用抗血小板药物 5(7.46) 2(9.52) 0.093 0.761 Lp(a)/(mg/L) 242.35±32.54 312.54±45.78 6.936 < 0.001 D-D/(mg/L) 0.89±0.18 0.95±0.12 1.373 0.175 UA/(μmol/L) 276.41±55.48 283.54±58.36 0.469 0.641  下载: 导出CSV
下载: 导出CSV
表 2 非再狭窄组和再狭窄组患者IVUS征象
Table 2. IVUS signs in the non-restenosis group and the restenosis group
例(%), X±S 项目 非再狭窄组(67例) 再狭窄组(21例) χ2/t P CAG显示钙化 25(37.31) 8(38.10) 0.036 0.850 IVUS钙化长度/mm 12.34±3.38 15.23±4.15 2.931 0.005 IVUS钙化分类 16.136 < 0.001 浅层/混合钙化 27(40.30) 19(90.48) 深层钙化 40(59.70) 2(9.52) 病变长度/mm 23.72±6.23 27.31±6.45 2.113 0.039 钙化特征评分 5.54±0.49 6.31±0.54 5.630 < 0.001 斑块形态学 PB>70% 38(56.72) 18(85.71) 5.810 0.016 MLA≤4 mm2 29(43.28) 15(71.43) 5.067 0.024 薄层纤维帽 8(11.94) 4(19.05) 0.686 0.408 钙化弧度 12.643 < 0.001 0°~90° 53(56.72) 8(33.33) 91°~360° 14(20.90) 13(61.90)
下载: 导出CSV
表 3 冠心病患者PCI术后1年内发生非靶血管再狭窄的危险因素
Table 3. Risk factors for non-target vessel restenosis in patients with coronary heart disease within 1 year after PCI
变量 β SE Wald χ2 OR 95%CI P 下限 上限 高脂血症 1.507 0.462 10.640 4.513 3.008 6.018 < 0.001 Lp(a) 1.413 0.458 9.518 4.108 2.481 5.736 < 0.001 钙化长度 1.024 0.406 6.361 2.784 1.331 4.238 0.016 浅层/混合钙化 1.887 0.512 13.583 6.600 4.778 8.421 < 0.001 病变长度 0.892 0.386 5.340 2.440 1.011 3.869 0.028 钙化特征评分 1.321 0.441 8.973 3.747 1.952 5.542 < 0.001 PB>70% 1.218 0.431 7.986 3.380 1.637 5.124 0.001 MLA≤4 mm2 1.105 0.415 7.090 3.019 1.386 4.652 0.008 钙化弧度91°~360° 1.789 0.501 12.751 5.983 3.984 7.983 < 0.001
下载: 导出CSV
-
[1] 莫睿, 吴强, 周瑜, 等. 冠心病患者外周血HOXA4基因表达及心血管病危险因素与冠心病病变特点的分析[J]. 临床心血管病杂志, 2024, 40(4): 291-295. doi: 10.13201/j.issn.1001-1439.2024.04.008
[2] Tao S, Tang X, Yu L, et al. Prognosis of coronary heart disease after percutaneous coronary intervention: a bibliometric analysis over the period 2004-2022[J]. Eur J Med Res, 2023, 28(1): 311. doi: 10.1186/s40001-023-01220-5
[3] Collet C, Munhoz D, Mizukami T, et al. Influence of pathophysiologic patterns of coronary artery disease on immediate percutaneous coronary intervention outcomes[J]. Circulation, 2024, 150(8): 586-597. doi: 10.1161/CIRCULATIONAHA.124.069450
[4] Duband B, Souteyrand G, Clerc JM, et al. Prevalence, Management and outcomes of percutaneous coronary intervention for coronary in-stent restenosis: insights from the France PCI registry[J]. Cardiovasc Revasc Med, 2023, 52: 39-46. doi: 10.1016/j.carrev.2023.02.006
[5] Koeda Y, Ishida M, Sasaki K, et al. Periprocedural and 30-day outcomes of robotic-assisted percutaneous coronary intervention used in the intravascular imaging guidance[J]. Cardiovasc Interv Ther, 2023, 38(1): 39-48. doi: 10.1007/s12928-022-00864-0
[6] Sonoda S, Node K. Intravascular ultrasound-guided percutaneous coronary intervention: practical application[J]. Interv Cardiol Clin, 2023, 12(2): 167-175.
[7] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 47(10): 766-783.
[8] Zhang Y, Liu P, Tang LJ, et al. Basing on the machine learning model to analyse the coronary calcification score and the coronary flow reserve score to evaluate the degree of coronary artery stenosis[J]. Comput Biol Med, 2023, 163: 107130. doi: 10.1016/j.compbiomed.2023.107130
[9] Saeed M, Stene LC, Reisæter AV, et al. End-stage renal disease: incidence and prediction by coronary heart disease, and educational level. Follow-up from diagnosis of childhood-onset type 1 diabetes throughout Norway 1973-2017[J]. Ann Epidemiol, 2022, 76: 181-187. doi: 10.1016/j.annepidem.2022.03.015
[10] Jafari A, Najafipour H, Shadkam M, et al. Evaluation of the novel three lipid indices for predicting five-and ten-year incidence of cardiovascular disease: findings from Kerman coronary artery disease risk factors study(KERCADRS)[J]. Lipids Health Dis, 2023, 22(1): 169. doi: 10.1186/s12944-023-01932-x
[11] Wang J, Yang Y, Zhang L, et al. Predictors of stent restenosis in Han and Uygur patients with coronary heart disease after PCI in the Xinjiang region[J]. Cardiol Res Pract, 2022: 7845108.
[12] Feng Q, Zhao Y, Wang H, et al. A predictive model involving serum uric acid, C-reactive protein, diabetes, hypercholesteremia, multiple lesions for restenosis risk in everolimus-eluting stent-treated coronary heart disease patients[J]. Front Cardiovasc Med, 2022, 9: 857922. doi: 10.3389/fcvm.2022.857922
[13] Li X, Ge Z, Kan J, et al. Intravascular ultrasound-guided versus angiography-guided percutaneous coronary intervention in acute coronary syndromes(IVUS-ACS): a two-stage, multicentre, randomised trial[J]. Lancet, 2024, 403(10439): 1855-1865. doi: 10.1016/S0140-6736(24)00282-4
[14] Baber U. Coronary artery calcification and mortality after revascularization: look beyond the heart[J]. JACC Cardiovasc Interv, 2022, 15(2): 205-207. doi: 10.1016/j.jcin.2021.11.008
[15] Tsuda M, Mizote I, Mukai T, et al. Aortic root rupture during balloon-expandable transcatheter aortic valve replacement in a patient without recognized risk factors for aortic root rupture: a case report[J]. Eur Heart J Case Rep, 2020, 4(3): 1-4.
[16] Dai N, Chen Z, Zhou F, et al. Association of lipoprotein(a)with coronary-computed tomography angiography-assessed high-risk coronary disease attributes and cardiovascular outcomes[J]. Circ Cardiovasc Imaging, 2022, 15(12): e014611.
[17] Meer R, Hoek AG, Bouman EJ, et al. Association between lower extremity arterial calcification and coronary arterial calcification in a population at increased risk of cardiovascular disease[J]. BMJ Open Diabetes Res Care, 2024, 12(1): e003811.
[18] Dastani M, Rahimi HR, Askari VR, et al. Three months of combination therapy with nano-curcumin reduces the inflammation and lipoprotein(a) in type 2 diabetic patients with mild to moderate coronary artery disease: Evidence of a randomized, double-blinded, placebo-controlled clinical trial[J]. Biofactors, 2023, 49(1): 108-118.
-
计量
- 文章访问数: 26
- 施引文献: 0