
-
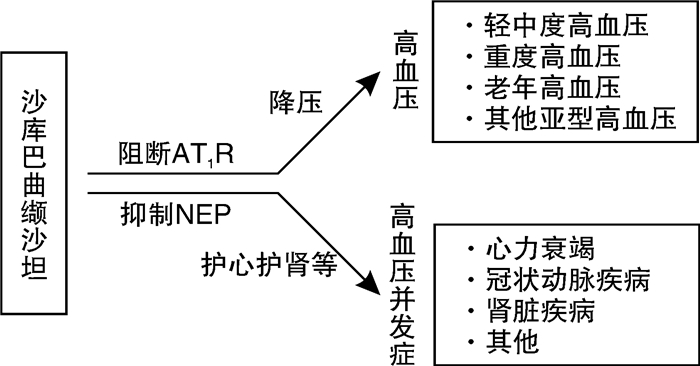
摘要: 血管紧张素受体-脑啡肽酶抑制剂(ARNI)是近些年推出的作用于射血分数减低型心力衰竭患者的一类新型药物,包含缬沙坦和沙库巴曲2种成分,可同时作用于肾素-血管紧张素-醛固酮系统(RAAS)和利钠肽系统(NPS),发挥利尿、利钠、舒张血管、拮抗RAAS等作用。新近研究发现,ARNI也可用于高血压治疗,对高血压及其并发症均有显著作用。本文就ARNI对高血压及其有关的心力衰竭、冠状动脉疾病及肾脏疾病等并发症的作用及地位作一综述。
-
关键词:
- 高血压 /
- 血管紧张素受体-脑啡肽酶抑制剂 /
- 并发症
Abstract: Angiotensin receptor-enkephalinase inhibitors (ARNIs) are the new type of drugs that act on heart failure with reduced ejection fraction. They contain two components, valsartan and sacubitril, which can act on both the renin-angiotensin-aldosterone system (RAAS) and the natriuretic peptide system (NPS). ARNI exerts diuretic, natriuretic, vasodilatory, and RAAS antagonistic effects. Recent studies have found that ARNI can also be used to treat hypertension and has a significant effect on hypertension and its complications. This article will review the role and status of ARNI in hypertension and its related complications such as heart failure, coronary artery disease, and renal disease.-
Key words:
- hypertension /
- angiotensin receptor-neprilysin inhibitor /
- complications
-

-
表 1 LCZ696与高血压等心血管疾病研究汇总
Table 1. The studies of LCZ696 in hypertension and cardiovascular diseases
研究类别 研究对象 样本量/例 年龄/岁 对照组 随访时间/周 主要结果 LCZ696不良事件发生率/% LCZ696与高血压相关研究 Ruilope等[13] 轻中度高血压 1328 18~75 缬沙坦和安慰剂 8 LCZ696对比相应剂量缬沙坦:血压平均降低4.20/2.17 mmHg(P < 0.05) < 30.00 Kario等[14] 轻中度高血压 389 ≥18 安慰剂 8 LCZ696血压控制率(<140/90 mmHg)为50%左右,显著高于安慰剂(15.2%) 约38.00 Supasyndh等[15] 轻中度高血压 341 ≥18 单臂 52 基于沙库巴曲/缬沙坦的降压方案总体血压控制率达75.3% 63.90 Wang等[16] 轻中度高血压 266 ≥18 安慰剂 8 与氨氯地平单药治疗相比,LCZ696/氨氯地平显著降低了24 h动态压(P < 0.001) 20.00 Kario等[17] 重度高血压 35 ≥18 单臂 8 第8周时血压降低达35.3/22.1 mmHg 48.60 Supasyndh等[19] 老年高血压 588 ≥65 奥美沙坦 14 第10周时LCZ696较奥美沙坦降压更明显(22.71 mmHg∶16.11 mmHg,P < 0.001) 47.60 Williams等[20] 老年收缩期高血压 454 ≥60 奥美沙坦 52 在降低动态中心主动脉收缩压和肱动脉收缩压方面LCZ696优于奥美沙坦(P < 0.001) 57.60 Wang等[22] 盐敏感高血压 72 ≥18 缬沙坦 8 LCZ696通过利尿利钠达到更好的血压控制作用,血压波动较小,夜间动态血压降低的尤为明显 32.40 LCZ696与高血压并发症等相关研究 Balmforth等[25] HFrEF 8399 ≥18 依那普利 108 LCZ696在降低心衰再住院率及全因死亡率方面显著优于依那普利,且不受病因影响 46.09 Solomon等[26] HFpEF 4822 ≥50 缬沙坦 140 与缬沙坦相比,LCZ696的主要结局事件较少,但无统计学差异;LCZ696降低了冠状动脉复合结局风险;LCZ696具有肾脏保护作用 58.87 Rezq等[31] STEMI 200 18~90 雷米普利 24 6个月时,LCZ696与雷米普利组主要心脏不良事件20%∶38%(OR=0.42,95%CI:0.23~0.78,P=0.005) 未观察到不良事件 Ito等[34] 高血压合并中重度肾功能不全 56 ≥20 单臂 8 LCZ696在日本高血压和肾功能不全患者中血压平均降低分别为20.5/8.3 mmHg,尿白蛋白/肌酐比平均降低为15.1% 43.80 Zhang等[36] 载脂蛋白E缺陷小鼠 72 / 对照组和缬沙坦组 12 LCZ696较对照组及缬沙坦组更能抑制炎症反应及动脉粥样硬化 / Martens等[38] HFrEF 151 未提及 单臂 52 LCZ696可减少室性心律失常的发生 / Jordan等[39] 肥胖高血压 98 ≥18 氨氯地平 8 LC696较氨氯地平更能增加外周胰岛素敏感性及腹部脂肪分解 60.00  下载: 导出CSV
下载: 导出CSV
-
[1] Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Circulation, 2018, 138(17): e426-e483.
[2] Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries[J]. Circulation, 2016, 134(6): 441-450. doi: 10.1161/CIRCULATIONAHA.115.018912
[3] Forouzanfar MH, Liu P, Roth GA, et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mmHg, 1990-2015[J]. JAMA, 2017, 317(2): 165-182. doi: 10.1001/jama.2016.19043
[4] Rapsomaniki E, Timmis A, George J, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people[J]. Lancet, 2014, 383(9932): 1899-1911. doi: 10.1016/S0140-6736(14)60685-1
[5] Oparil S, Acelajado MC, Bakris GL, et al. Hypertension[J]. Nat Rev Dis Primers, 2018, 4: 18014. doi: 10.1038/nrdp.2018.14
[6] Volpe M, Rubattu S, Burnett J Jr. Natriuretic peptides in cardiovascular diseases: current use and perspectives[J]. Eur Heart J, 2014, 35(7): 419-425. doi: 10.1093/eurheartj/eht466
[7] Lin LM, Wu Y, Wu MF, et al. Focus on the Novel Cardiovascular Drug LZC696: from Evidence to Clinical Consideration[J]. Cardiovasc Drugs Ther, 2016, 30(6): 623-633. doi: 10.1007/s10557-016-6699-5
[8] von Lueder TG, Atar D, Krum H. Current role of neprilysin inhibitors in hypertension and heart failure[J]. Pharmacol Ther, 2014, 144(1): 41-49. doi: 10.1016/j.pharmthera.2014.05.002
[9] Rubattu S, Forte M, Marchitti S, et al. Molecular Implications of Natriuretic Peptides in the Protection from Hypertension and Target Organ Damage Development[J]. Int J Mol Sci, 2019, 20(4).
[10] Hubers SA, Brown NJ. Combined Angiotensin Receptor Antagonism and Neprilysin Inhibition[J]. Circulation, 2016, 133(11): 1115-1124. doi: 10.1161/CIRCULATIONAHA.115.018622
[11] 中国高血压联盟《动态血压监测指南》委员会. 2020中国动态血压监测指南[J]. 中国循环杂志, 2021, 36(4): 313-328. doi: 10.3969/j.issn.1000-3614.2021.04.001
[12] 中国医疗保健国际交流促进会高血压分会, 中国医师协会心血管分会, 中国高血压联盟, 等. 沙库巴曲缬沙坦在高血压患者临床应用的中国专家建议[J]. 中华高血压杂志, 2021, 29(2): 108-114. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ202102006.htm
[13] Ruilope LM, Dukat A, Böhm M, et al. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin Ⅱ receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study[J]. Lancet, 2010, 375(9722): 1255-1266. doi: 10.1016/S0140-6736(09)61966-8
[14] Kario K, Sun N, Chiang FT, et al. Efficacy and safety of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor, in Asian patients with hypertension: a randomized, double-blind, placebo-controlled study[J]. Hypertension, 2014, 63(4): 698-705. doi: 10.1161/HYPERTENSIONAHA.113.02002
[15] Supasyndh O, Sun N, Kario K, et al. Long-term(52-week)safety and efficacy of Sacubitril/valsartan in Asian patients with hypertension[J]. Hypertens Res, 2017, 40(5): 472-476. doi: 10.1038/hr.2016.151
[16] Wang JG, Yukisada K, Sibulo A Jr, et al. Efficacy and safety of sacubitril/valsartan(LCZ696) add-on to amlodipine in Asian patients with systolic hypertension uncontrolled with amlodipine monotherapy[J]. J Hypertens, 2017, 35(4): 877-885. doi: 10.1097/HJH.0000000000001219
[17] Kario K, Tamaki Y, Okino N, et al. LCZ696, a First-in-Class Angiotensin Receptor-Neprilysin Inhibitor: The First Clinical Experience in Patients With Severe Hypertension[J]. J Clin Hypertens(Greenwich), 2016, 18(4): 308-314. doi: 10.1111/jch.12667
[18] Dao HH, Essalihi R, Bouvet C, et al. Evolution and modulation of age-related medial elastocalcinosis: impact on large artery stiffness and isolated systolic hypertension[J]. Cardiovasc Res, 2005, 66(2): 307-317. doi: 10.1016/j.cardiores.2005.01.012
[19] Supasyndh O, Wang J, Hafeez K, et al. Efficacy and Safety of Sacubitril/Valsartan(LCZ696) Compared With Olmesartan in Elderly Asian Patients(≥65 Years)With Systolic Hypertension[J]. Am J Hypertens, 2017, 30(12): 1163-1169. doi: 10.1093/ajh/hpx111
[20] Williams B, Cockcroft JR, Kario K, et al. Effects of Sacubitril/Valsartan Versus Olmesartan on Central Hemodynamics in the Elderly With Systolic Hypertension: The PARAMETER Study[J]. Hypertension, 2017, 69(3): 411-420. doi: 10.1161/HYPERTENSIONAHA.116.08556
[21] Yenerçaǧ M, Arslan U, Dereli S, et al. Effects of angiotensin receptor neprilysin inhibition on pulmonary arterial stiffness in heart failure with reduced ejection fraction[J]. Int J Cardiovasc Imaging, 2021, 37(1): 165-173. doi: 10.1007/s10554-020-01973-8
[22] Wang TD, Tan RS, Lee HY, et al. Effects of Sacubitril/Valsartan(LCZ696) on Natriuresis, Diuresis, Blood Pressures, and NT-proBNP in Salt-Sensitive Hypertension[J]. Hypertension, 2017, 69(1): 32-41. doi: 10.1161/HYPERTENSIONAHA.116.08484
[23] Kjeldsen SE, Narkiewicz K, Burnier M, et al. Will we ever use angiotensin receptor neprilysin inhibition(ARNi)for the treatment of hypertension?[J]. Blood Press, 2019, 28(2): 75-76. doi: 10.1080/08037051.2019.1584975
[24] Cannon JA, Shen L, Jhund PS, et al. Dementia-related adverse events in PARADIGM-HF and other trials in heart failure with reduced ejection fraction[J]. Eur J Heart Fail, 2017, 19(1): 129-137. doi: 10.1002/ejhf.687
[25] Balmforth C, Simpson J, Shen L, et al. Outcomes and Effect of Treatment According to Etiology in HFrEF: An Analysis of PARADIGM-HF[J]. JACC Heart Fail, 2019, 7(6): 457-465. doi: 10.1016/j.jchf.2019.02.015
[26] Solomon SD, McMurray J, Anand IS, et al. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction[J]. N Engl J Med, 2019, 381(17): 1609-1620. doi: 10.1056/NEJMoa1908655
[27] Selvaraj S, Claggett BL, Böhm M, et al. Systolic Blood Pressure in Heart Failure With Preserved Ejection Fraction Treated With Sacubitril/Valsartan[J]. J Am Coll Cardiol, 2020, 75(14): 1644-1656. doi: 10.1016/j.jacc.2020.02.009
[28] 廖玉华, 杨杰孚, 张健, 等. 舒张性心力衰竭诊断和治疗专家共识[J]. 临床心血管病杂志, 2020, 36(1): 1-10. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202001001.htm
[29] Mogensen UM, Køber L, Jhund PS, et al. Sacubitril/valsartan reduces serum uric acid concentration, an independent predictor of adverse outcomes in PARADIGM-HF[J]. Eur J Heart Fail, 2018, 20(3): 514-522.
[30] von Lueder TG, Wang BH, Kompa AR, et al. Angiotensin receptor neprilysin inhibitor LCZ696 attenuates cardiac remodeling and dysfunction after myocardial infarction by reducing cardiac fibrosis and hypertrophy[J]. Circ Heart Fail, 2015, 8(1): 71-78.
[31] Rezq A, Saad M, El Nozahi M. Comparison of the Efficacy and Safety of Sacubitril/Valsartan versus Ramipril in Patients With ST-Segment Elevation Myocardial Infarction[J]. Am J Cardiol, 2021, 143: 7-13.
[32] Ishii M, Kaikita K, Sato K, et al. Cardioprotective Effects of LCZ696(Sacubitril/Valsartan)After Experimental Acute Myocardial Infarction[J]. JACC Basic Transl Sci, 2017, 2(6): 655-668.
[33] Damman K, Gori M, Claggett B, et al. Renal Effects and Associated Outcomes During Angiotensin-Neprilysin Inhibition in Heart Failure[J]. JACC Heart Fail, 2018, 6(6): 489-498.
[34] Ito S, Satoh M, Tamaki Y, et al. Safety and efficacy of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor, in Japanese patients with hypertension and renal dysfunction[J]. Hypertens Res, 2015, 38(4): 269-275.
[35] Judge P, Haynes R, Landray MJ, et al. Neprilysin inhibition in chronic kidney disease[J]. Nephrol Dial Transplant, 2015, 30(5): 738-743.
[36] Zhang H, Liu G, Zhou W, et al. Neprilysin Inhibitor-Angiotensin Ⅱ Receptor Blocker Combination Therapy(Sacubitril/valsartan)Suppresses Atherosclerotic Plaque Formation and Inhibits Inflammation in Apolipoprotein E-Deficient Mice[J]. Sci Rep, 2019, 9(1): 6509.
[37] Sarrias A, Bayes-Genis A. Is Sacubitril/Valsartan(Also)an Antiarrhythmic Drug?[J]. Circulation, 2018, 138(6): 551-553.
[38] Martens P, Nuyens D, Rivero-Ayerza M, et al. Sacubitril/valsartan reduces ventricular arrhythmias in parallel with left ventricular reverse remodeling in heart failure with reduced ejection fraction[J]. Clin Res Cardiol, 2019, 108(10): 1074-1082.
[39] Jordan J, Stinkens R, Jax T, et al. Improved Insulin Sensitivity With Angiotensin Receptor Neprilysin Inhibition in Individuals With Obesity and Hypertension[J]. Clin Pharmacol Ther, 2017, 101(2): 254-263.
-
图(1)
表(1)
计量
- 文章访问数: 7273
- PDF下载数: 2978
- 施引文献: 0