
Status of secondary preventive antiplatelet and statin therapy for coronary heart disease and ischemic stroke in central China
-
摘要: 目的 评估中国华中地区社区居民中既往患有冠心病和缺血性脑卒中人群的二级预防抗血小板和他汀治疗情况,分析个体特征与用药的关联关系。方法 本研究利用2015年9月—2019年11月中国华中地区3个省份心血管病高危人群早期筛查与综合干预项目采集数据,选取35~75岁常住居民,通过问卷调查收集患病及药物使用情况。采用多变量混合效应模型评估个体特征与二级预防用药的相关性。结果 在414 209例调查对象中,自报患有冠心病、缺血性脑卒中史的比例为3.2%。在这些患者中,报告使用抗血小板药物、他汀类药物的比例为29.4%。多因素分析结果显示,女性、既往诊断心血管病>7年的调查对象使用抗血小板药物、他汀类药物的可能性更低。结论 中国华中地区冠心病和缺血性脑卒中患者人群目前二级预防用药情况不太理想。本研究明确了华中地区主要心血管病防控的靶点人群,便于制定针对性二级预防干预措施。Abstract: Objective To explore the current use of secondary prevention antiplatelet and statin therapy among community residents with established coronary heart disease(CHD) and ischemic stroke(IS) in central China, and to identify its associated individual characteristics.Methods his study was based on the data collected from the early screening and comprehensive intervention program for high-risk population of cardiovascular disease in 3 provinces in central China from September 2015 to November 2019. Permanent residents aged 35 to 75 were selected and their disease and drug use were collected through a questionnaire survey. Multivariable mixed models were fitted to assess the associations of individual characteristics with the reported use of secondary prevention therapies.Results Among 414 209 participants, 3.2% reported a history of CHD and/or IS. Among these patients, 29.4% reported using antiplatelet drugs and statins. Multivariate analysis showed that women and subjects with a prior diagnosis of cardiovascular disease > 7 years were less likely to use antiplatelet drugs or statins.Conclusion The current situation of secondary preventive drug use in patients with coronary heart disease and ischemic stroke in central China is not ideal. Our study identifies target populations, tailored interventions to improve secondary prevention of cardiovascular diseases.
-
Key words:
- coronary heart disease /
- central China /
- ischemic stroke /
- antiplatelet drugs /
- statins
-

-
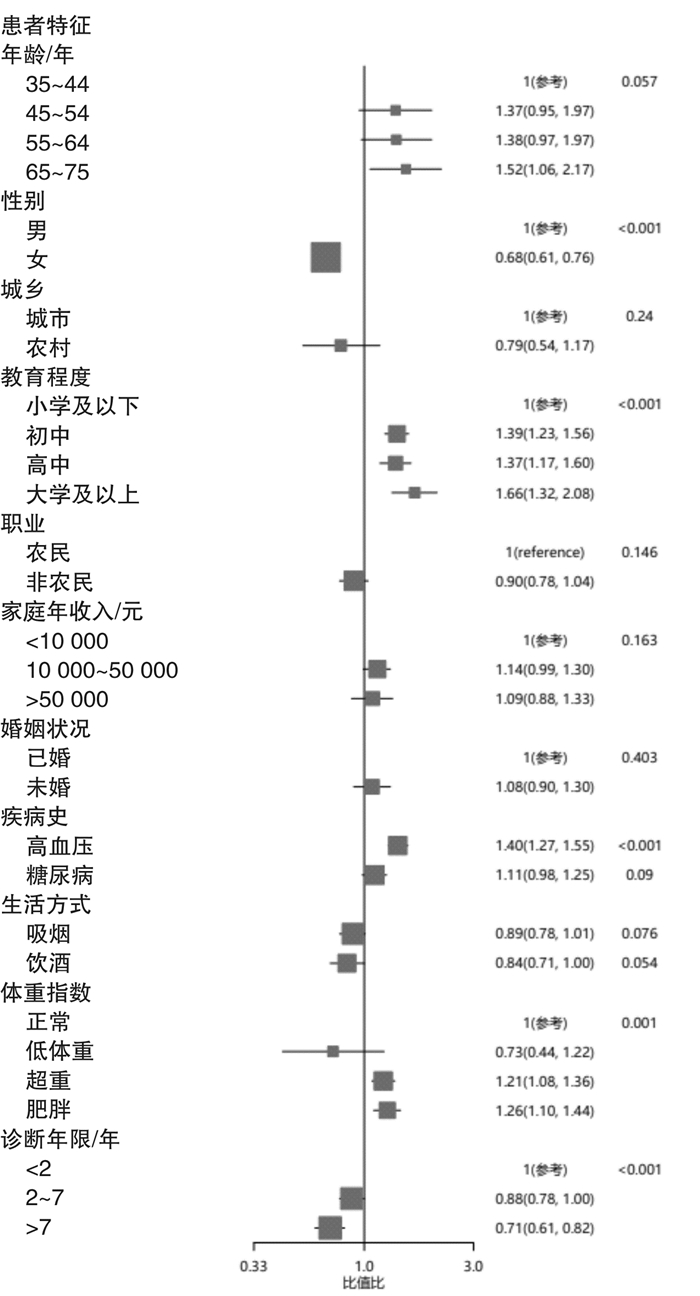
图 1 多变量回归模型评估个体特征与报告使用抗血小板药物或他汀类药物之间的相关关系
Figure 1. Multivariable regression model for association between individual characteristics and the reported use of antiplatelet drugs or statins
表 1 CHD、IS患者基本特征
Table 1. Baseline characteristics of participants with CHD and/or IS
例(%), X±S 项目 仅患有CHD 仅患有IS 同时患有CHD和IS 患有CHD和(或)IS 人数/例 5261 7405 384 13050 年龄/岁 62.2±8.1 62.3±7.5 64.3±7.4 62.3±7.8 年龄 35~44岁 156(3.0) 119(1.6) 3(0.8) 278(2.1) 45~54岁 838(15.9) 1150(15.5) 46(12.0) 2034(15.6) 55~64岁 1915(36.4) 2915(39.4) 117(30.5) 4947(37.9) 65~75岁 2352(44.7) 3221(43.5) 218(56.8) 5791(44.4) 性别 男 2955(56.2) 3562(48.1) 206(53.6) 6723(51.5) 女 2306(43.8) 3843(51.9) 178(46.4) 6327(48.5) 城乡 城市 1987(37.8) 2753(37.2) 193(50.3) 4933(37.8) 农村 3274(62.2) 4652(62.8) 191(49.7) 8117(62.2) 教育程度 小学及以下 2295(45.1) 3646(50.9) 164(42.7) 6105(48.3) 初中 1566(30.8) 2132(29.7) 117(30.5) 3815(30.2) 高中 804(15.8) 1027(14.3) 61(15.9) 1892(15.0) 大学及以上 318(6.3) 306(4.3) 29(7.6) 653(5.2) 不清楚 102(2.0) 59(0.8) 6(1.6) 167(1.3) 职业 农民 2337(44.4) 3665(49.5) 139(36.2) 6141(47.1) 非农民 2816(53.5) 3664(49.5) 240(62.5) 6720(51.5) 不清楚 108(2.1) 76(1.0) 5(1.3) 189(1.4) 家庭年收入 < 10 000元 1002(19) 1612(21.8) 72(18.8) 2686(20.6) 10 000~50 000元 3188(60.6) 4540(61.3) 247(64.3) 7975(61.1) >50 000元 746(14.2) 885(12.0) 50(13.0) 1681(12.9) 不清楚 325(6.2) 368(5.0) 15(3.9) 708(5.4) 婚姻状况 已婚 4810(91.4) 6670(90.1) 342(89.1) 11822(90.6) 丧偶、分居、离婚、单身 380(7.2) 680(9.2) 32(8.3) 1092(8.4) 不清楚 71(1.3) 55(0.7) 10(2.6) 136(1.0) 生活方式 吸烟 1100(20.9) 1478(20.0) 70(18.2) 2648(20.3) 饮酒 460(8.7) 586(7.9) 31(8.1) 1077(8.3) 疾病史 高血压史 2402(45.7) 4137(55.9) 260(67.7) 6799(52.1) 糖尿病史 986(18.7) 1192(16.1) 112(29.2) 2290(17.5) BMI分组 低体重 73(1.4) 84(1.1) 6(1.6) 163(1.2) 正常体重 1701(32.3) 2425(32.7) 92(24.0) 4218(32.3) 超重 2316(44.0) 3315(44.8) 188(49.0) 5819(44.6) 肥胖 1171(22.3) 1581(21.4) 98(25.5) 2850(21.8) 诊断年限 < 2年 883(18.9) 1167(17.9) 79(21.9) 2129(18.4) 2~7年 2849(61.1) 3908(60.0) 211(58.4) 6968(60.4) >7年 934(20.0) 1440(22.1) 71(19.7) 2445(21.2)  下载: 导出CSV
下载: 导出CSV
表 2 CHD、IS患者的抗血小板药物或他汀类药物使用情况
Table 2. Use of antiplatelet drugs or statins among participants with CHD and/or IS
药物使用情况 仅患CHD 仅患IS 同时患有CHD和IS 患有CHD或IS P值 例(%) 95%CI 例(%) 95%CI 例(%) 95%CI 例(%) 95%CI 使用抗血小板药物或他汀类药物 1641 (31.2) 29.9~ 32.5 2029 (27.4) 26.4~ 28.4 172 (44.8) 39.7~ 49.9 3842 (29.4) 28.7~ 30.2 < 0.001 仅使用抗血小板药物 1378 (26.2) 25.0~ 27.4 1722 (23.3) 22.3~ 24.2 142 (37.0) 32.1~ 42.0 3242 (24.8) 24.1~ 25.6 < 0.001 仅使用他汀类药物 1058 (20.1) 19.0~ 21.2 1095 (14.8) 14.0~ 15.6 112 (29.2) 24.7~ 34.0 2265 (17.4) 16.7~ 18.0 < 0.001 同时使用抗血小板药和他汀类药物 795 (15.1) 14.2~ 16.1 788 (10.6) 10.0~ 11.4 82 (21.4) 17.4~ 25.8 1665 (12.8) 12.2~ 13.3 < 0.001
下载: 导出CSV
表 3 使用抗血小板药物或他汀类药物的CHD、IS患者特征
Table 3. Use of antiplatelet drugs or statins among participants with CHD and/or IS by individual characteristics
例(%) 项目 仅患有CHD 仅患有IS 同时患有CHD和IS 患有CHD或IS P值 年龄 0.53 35~44岁 47(30.1) 28(23.5) 1(33.3) 76(27.3) 45~54岁 259(30.9) 330(28.7) 20(43.5) 609(29.9) 55~64岁 618(32.3) 811(27.8) 53(45.3) 1482(30.0) 65~75岁 717(30.5) 860(26.7) 98(45.0) 1675(28.9) 性别 < 0.001 男 1087(36.8) 1070(30.0) 107(51.9) 2264(33.7) 女 554(24.0) 959(25.0) 65(36.5) 1578(24.9) 城乡 < 0.001 城市 839(42.2) 869(31.6) 94(48.7) 1802(36.5) 农村 802(24.5) 1160(24.9) 78(40.8) 2040(25.1) 教育程度 < 0.001 小学及以下 489(21.3) 807(22.1) 56(34.2) 1352(22.2) 初中 561(35.8) 704(33.0) 62(53.0) 1327(34.8) 高中 342(42.5) 330(32.1) 37(60.7) 709(37.5) 大学及以上 154(48.4) 99(32.4) 15(51.7) 268(41.0) 职业 < 0.001 农民 520(22.3) 861(23.5) 54(38.9) 1435(23.4) 非农民 1090(38.7) 1147(31.3) 118(49.2) 2355(35.0) 家庭年收入 < 0.001 <10 000元 245(24.5) 457(28.4) 27(37.5) 729(27.1) 10 000~50 000元 1074(33.7) 1275(28.1) 112(45.3) 2461(30.9) >50 000元 234(31.4) 199(22.5) 29(58.0) 462(27.5) 婚姻状况 0.017 已婚 1514(31.5) 1844(27.7) 156(45.6) 3514(29.7) 未婚 104(27.4) 169(24.9) 14(43.8) 287(26.3) 高血压史 < 0.001 是 831(34.6) 1345(32.51) 124(47.7) 2300(33.8) 否 810(28.3) 684(20.9) 48(38.7) 1542(24.7) 糖尿病史 < 0.001 是 355(36.0) 373(31.3) 51(45.5) 779(34.0) 否 1286(30.1) 1656(26.7) 121(44.5) 3063(28.5) 吸烟 0.26 是 375(34.1) 402(27.2) 26(37.1) 803(30.3) 否 1266(30.4) 1627(27.5) 146(46.5) 3039(29.2) 饮酒 0.30 是 162(35.2) 159(27.1) 11(35.5) 332(30.8) 否 1479(30.8) 1870(27.4) 161(45.6) 3510(29.3) BMI分组 < 0.001 低体重 13(17.8) 12(14.3) 1(16.7) 26(16.0) 正常体重 430(25.3) 559(23.1) 43(46.7) 1032(24.5) 超重 767(33.1) 964(29.1) 87(46.3) 1818(31.2) 肥胖 431(36.8) 494(31.3) 41(41.8) 966(33.9) 诊断年限 0.68 <2年 298(33.8) 333(28.5) 35(44.3) 666(31.3) 2~7年 913(32.1) 1036(26.5) 96(45.5) 2045(29.4) >7年 245(26.2) 416(28.9) 28(39.4) 689(28.2)
下载: 导出CSV
-
[1] 国家心血管病中心. 中国心血管病报告2017[R]. 北京: 大百科全书出版社, 2017.
[2] Wang W, Jiang B, Sun H, et al. Prevalence, Incidence, and Mortality of Stroke in China: Results from a Nationwide Population-Based Survey of 480 687 Adults[J]. Circulation, 2017, 135(8): 759-771. doi: 10.1161/CIRCULATIONAHA.116.025250
[3] Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: a nationwide population-based cohort study[J]. Lancet Public Health, 2020, 5(12): e672-e681.
[4] Afilalo J, Duque G, Steele R, et al. Statins for secondary prevention in elderly patients: a hierarchical bayesian meta-analysis[J]. J Am Coll Cardiol, 2008, 51(1): 37-45. doi: 10.1016/j.jacc.2007.06.063
[5] Antithrombotic Trialists'(ATT)Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials[J]. Lancet, 2009, 373(9678): 1849-1860. doi: 10.1016/S0140-6736(09)60503-1
[6] 李悦, 石静, 何美娇. 急性冠状动脉综合征患者抗栓降阶治疗研究进展[J]. 临床心血管病杂志, 2020, 36(12): 1075-1078. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202012002.htm
[7] Wang YJ, Zhang SM, Zhang L, et al. Chinese guidelines for the secondary prevention of ischemic stroke and transient ischemic attack 2010[J]. CNS Neurosci Ther, 2012, 18(2): 93-101. doi: 10.1111/j.1755-5949.2011.00290.x
[8] Wang Y, Liu M, Pu C. 2014 Chinese guidelines for secondary prevention of ischemic stroke and transient ischemic attack[J]. Int J Stroke, 2017, 12(3): 302-320. doi: 10.1177/1747493017694391
[9] 中华医学会心血管病学分会, 中国康复医学会心血管病专业委员会, 中国老年学学会心脑血管病专业委员会. 冠心病康复与二级预防中国专家共识[J]. 中华心血管病杂志, 2013, 41(4): 267-275. doi: 10.3760/cma.j.issn.0253-3758.2013.04.003
[10] Lu J, Xuan S, Downing NS, et al. Protocol for the China peace(patient-centered Evaluative assessment of cardiac events)million persons project pilot[J]. BMJ Open, 2016, 6(1): e010200. doi: 10.1136/bmjopen-2015-010200
[11] James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee(JNC 8)[J]. JAMA, 2014, 311(5): 507-520. doi: 10.1001/jama.2013.284427
[12] Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report[J]. JAMA, 2003, 289(19): 2560-2572. doi: 10.1001/jama.289.19.2560
[13] Zhou BF, Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults[J]. Biomed Environ Sci, 2002, 15(1): 83-96.
[14] Lu J, Zhang L, Lu Y, et al. Secondary prevention of cardiovascular disease in China[J]. Heart, 2020, 106(17): 1349-1356.
[15] Chen Y, Li L, Zhang Q, et al. Use of drug treatment for secondary prevention of cardiovascular disease in urban and rural communities of China: China Kadoorie Biobank Study of 0.5 million people[J]. Int J Cardiol, 2014, 172(1): 88-95.
[16] 刘军, 赵冬, 刘静, 等. 阿司匹林在冠心病二级预防中的应用现况[J]. 中华内科杂志, 2009, 48(10): 809-813.
[17] 宋波, 杨光, 高远, 等. 他汀类药物在缺血性卒中和短暂性脑缺血发作二级预防中的应用现状及其依从性[J]. 中华神经科杂志, 2012, 45(2): 107-111.
-
图(1)
表(3)
计量
- 文章访问数: 1006
- PDF下载数: 631
- 施引文献: 0