
Construction and external validation of a risk-prediction model for cardiac rupture after acute myocardial infarction
-
摘要: 目的 回顾性分析急性心肌梗死(AMI)后心脏破裂(CR)患者的临床特征及危险因素,并构建实用风险预测模型并进行独立的外部验证。方法 从南昌大学第一附属医院及南昌大学附属人民医院数据库中选取2013年1月—2020年9月的急性ST段抬高型心肌梗死(STEMI)CR患者126例和非CR患者339例,将南昌大学附属人民医院纳入的患者作为建模组(CR组:86例,非CR组:228例),南昌大学第一附属医院纳入的患者作为验证组(CR组:40例,非CR组:111例)。采用单因素分析和多因素logistic回归分析得出CR的危险因素,根据各危险因素的加权赋分建立CR风险预测模型,通过受试者工作特征(ROC)曲线下面积(AUC)及Hosmer-Lemeshow检验检测模型的区分度和校准度,并在验证组中检验该模型的价值。结果 建模组中多因素logistic回归分析结果显示:年龄≥63岁(OR=2.446,95%CI:1.017~5.881,P=0.046)、女性(OR=2.614,95%CI:1.155~5.917,P=0.021)、收缩压≤120 mmHg(OR=2.569,95%CI:1.121~5.887,P=0.026)、心率≥100次/min(OR=2.532,95%CI:1.055~6.073,P=0.037)、中性粒细胞百分比/白蛋白(NPAR)≥2.2(OR=3.328,95%CI:1.463~7.570,P=0.004)、肌酐≥106μmol/L(OR=2.744,95%CI:1.178~6.392,P=0.019)、Ca2+≤2.2 mmol/L(OR=3.059,95%CI:1.369~6.835,P=0.006)、行急诊PCI(OR=0.442,95%CI:0.198~0.989,P=0.047)、口服β受体阻滞剂(OR=0.268,95%CI:0.118~0.607,P=0.002)是CR的独立影响因素。基于这9个影响因素进行加权后建立了预测模型,总分为9分,患者评分≤4分归为低风险和评分≥5分归为高风险。本研究预测模型的AUC(0.906,95%CI:0.865~0.948,P< 0.001),Hosmer-Lemeshow检验(χ2=14.297,P>0.05),外部验证中AUC(0.785,95%CI:0.696~0.875,P< 0.001),Hosmer-Lemeshow检验(χ2=1.7,P=0.989),结果表明本研究模型对CR有较好的预测价值。结论 高龄、女性、收缩压低、心率快、NPAR升高、肌酐升高、Ca2+浓度降低是AMI后CR的危险因素,行急诊PCI、口服β受体阻滞剂是其保护因素,基于这9个变量建立了CR的风险预测模型,为一线临床医务工作者早期识别高危CR患者,积极实施干预措施,制定正确治疗决策提供了一定的参考依据。Abstract: Objective To explore the clinical characteristics and risk factors of patients with cardiac rupture(CR) after acute myocardial infarction(AMI) through retrospective research, and construct a practical risk-prediction model with independent external validation.Methods A total of 126 CR patients with AMI were selected from the databases of the First Affiliated Hospital of Nanchang University and the Jiangxi Provincial People's Hospital Affiliated to Nanchang University from January 2013 to September 2020, and 339 patients with non-CR were enrolled. The patients included in the Jiangxi Provincial People's Hospital Affiliated to Nanchang University were used as the modeling group (CR group: n=86, non-CR group: n=228), and the patients in the First Affiliated Hospital of Nanchang University were treated as the verification group (CR group: n=40, non-CR group: n=111). The risk factors of CR were obtained by univariable and multivariable logistic regression analysis. According to the weighted scores of each independent risk factor, the CR risk-prediction model was established. The discrimination and calibration of the model were detected by the area under the curve(AUC)of the receiver operating characteristic(ROC) and Hosmer-Lemeshow test, respectively. The value of the model was examined by the validation group.Results The results of the multivariate logistic regression analysis showed that the age≥63 years old(OR=2.446, 95%CI: 1.017-5.881,P=0.046), female (OR=2.614, 95%CI: 1.155-5.917,P=0.021), systolic blood pressure≤120mmHg(OR=2.569, 95%CI: 1.121-5.887,P=0.026), heart rate≥100 times/min (OR=2.532, 95%CI:1.055-6.073,P=0.037), neutrophil percentage to albumin ratio(NPAR)≥2.2(OR=3.328, 95%CI: 1.463-7.57,P=0.004), creatinine≥106μmol/L(OR=2.744, 95%CI: 1.178-6.392,P=0.019), calcium concentration≤2.2 mmol/L(OR=3.059, 95%CI: 1.369-6.835,P=0.006), emergency PCI(OR=0.442, 95%CI: 0.198~0.989,P=0.047) and oral beta blockers(OR=0.268, 95%CI: 0.118-0.607,P=0.002) were independent risk factors for CR after AMI. Based on the weighting of these nine risk factors, a predicting model was established with a total score of 9. The patient score≤4 was classified as low risk and the score≥5 was assigned to high risk. The results of the predicting model with AUC of 0.906(95%CI: 0.865-0.948,P< 0.001) and Hosmer-Lemeshow test (χ2=14.297,P> 0.05), external validation with AUC of 0.785 (95%CI: 0.696-0.875,P< 0.001) and Hosmer-Lemeshow test (χ2=1.7,P=0.989) demonstrated that the risk-prediction model had a good predictive value for CR.Conclusion Advanced age, female, low systolic blood pressure, rapid heart rate, elevated NPAR, increased creatinine, and decreased calcium concentration were the independent risk factors for CR after AMI, while emergency PCI and oral beta blockers were the protective factors. Based on these nine variables, a risk-prediction model of CR after AMI was established.
-
Key words:
- acute myocardial infarction /
- cardiac rupture /
- risk prediction model /
- risk factor
-

-
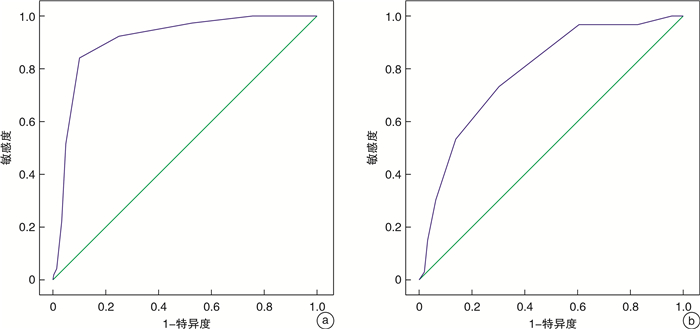
图 1 建模组(a)和验证组(b)预测CR模型的ROC曲线
Figure 1. The ROC curve of predicting CR in modeling group (a) and verification group (b)
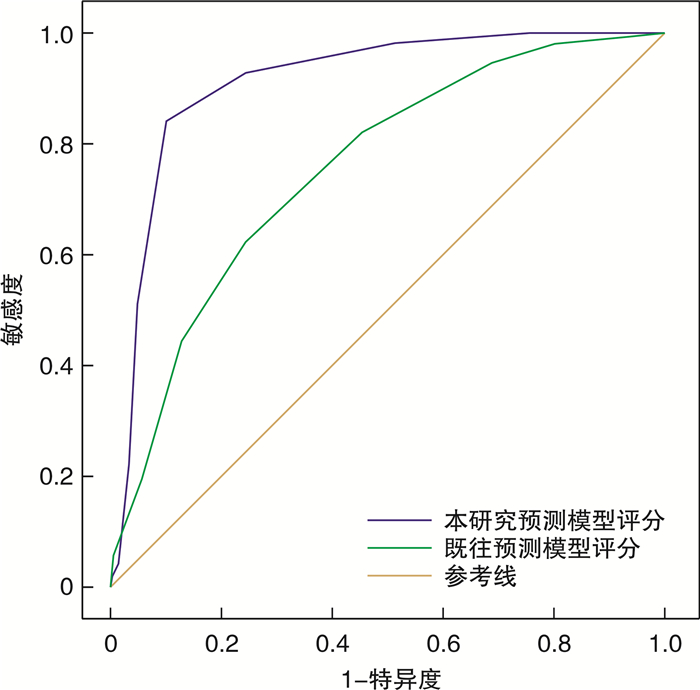
图 2 本模型与既往CR模型ROC曲线比较
Figure 2. Comparison of ROC curve between this model and previous model
表 1 建模组患者一般资料比较
Table 1. Comparison of general datas of patients in modeling group
例(%), M(Q1, Q3), X±S 指标 CR组(86例) 非CR组(228例) P值 年龄/岁 70.80±9.55 61.69±12.58 < 0.001 女性 41(47.7) 63(27.6) 0.001 收缩压/mmHg 118.65±23.79 131.57±23.43 < 0.001 舒张压/mmHg 71.16±14.99 74.58±12.72 0.046 心率/(次·min-1) 90.30±21.68 81.84±17.92 0.001 高血压史 51(59.3) 124(54.4) 0.434 糖尿病史 22(25.6) 59(25.9) 0.957 脑卒中史 8(9.3) 15(6.6) 0.409 吸烟史 31(36.0) 106(46.5) 0.096 饮酒史 15(17.4) 56(24.6) 0.179 症状发生到就诊时间/h 12(6,24) 8(5,15) 0.053 合并恶性心律失常 17(19.8) 15(6.6) < 0.001 Killip分级 < 0.001 Ⅰ~Ⅱ 66(76.7) 212(93.0) Ⅲ~Ⅳ 20(23.3) 16(7.0) 急诊PCI 27(31.4) 123(53.9) < 0.001 罪犯血管 0.796 前降支 28(59.6) 127(60.8) 回旋支 8(17.0) 28(13.4) 右冠 11(23.4) 54(25.8) 白细胞计数/(×109·L-1) 12.23(9.75,15.35) 8.85(6.58,11.48) < 0.001 中性粒细胞百分比/% 83.35(77.90,87.00) 74.60(65.40,83.60) < 0.001 白蛋白/(g·L-1) 34.67±4.35 40.42±4.94 < 0.001 NPAR 2.43(2.08,2.67) 1.78(1.54,2.06) < 0.001 肌酐/(μmol·L-1) 94.00(74.75,144.25) 77.95(63.98,92.73) < 0.001 尿酸/(μmol·L-1) 413.50(298.25,511.25) 353.00(289.00,416.00) 0.012 CK/(U·L-1) 608.00(277.00,1769.00) 315.00(111.25,761.50) < 0.001 CK-MB/(U·L-1) 64.00(31.00,162.25) 40.50(20.00,87.50) 0.005 cTnI/(μg·L-1) 14.00(6.00,24.85) 0.32(0.01,2.60) < 0.001 K+/(mmol·L-1) 4.00(3.73,4.40) 4.02(3.69,4.34) 0.823 Ca2+/(mmol·L-1) 2.14(2.04,2.24) 2.27(2.16,2.37) < 0.001 溶栓 6(7.0) 2(0.9) 0.008 ACEI/ARB 13(15.1) 114(50.0) < 0.001 他汀类药物 79(91.9) 222(97.4) 0.062 β受体阻滞剂 19(22.1) 140(61.4) < 0.001 注:1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 建模组多因素logistic回归分析结果
Table 2. Results of multivariate logistic regression analysis in the modeling group
变量 β P OR 95%CI 年龄≥63岁 0.894 0.046 2.446 1.017~5.881 女性 0.961 0.021 2.614 1.155~5.917 NPAR≥2.2 1.202 0.004 3.328 1.463~7.570 收缩压≤120 mmHg 0.944 0.026 2.569 1.121~5.887 溶栓 1.390 0.208 4.015 0.461~14.937 心率≥100次/min 0.929 0.037 2.532 1.055~6.073 肌酐≥106 μmol/L 1.009 0.019 2.744 1.178~6.392 Ca2+≤2.2 mmol/L 1.118 0.006 3.059 1.369~6.835 急诊PCI -0.815 0.047 0.442 0.198~0.989 口服β受体阻滞剂 -1.316 0.002 0.268 0.118~0.607 合并恶性心律失常 1.036 0.068 2.819 0.928~8.565
下载: 导出CSV
-
[1] Zhao D, Liu J, Wang M, et al. Epidemiology of cardiovascular disease in China: current features and implications[J]. Nat Rev Cardiol, 2019, 16(4): 203-212. doi: 10.1038/s41569-018-0119-4
[2] Roberts WC. Cardiac rupture during acute myocardial infarction diagnosed clinically[J]. Coron Artery Dis, 2018, 29(2): 95-96. doi: 10.1097/MCA.0000000000000586
[3] 王玉辉, 童路, 帅欣欣. 急性心肌梗死合并游离壁破裂的早期预警[J]. 临床心血管病杂志, 2021, 37(10): 891-895. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202110004.htm
[4] 肖文涛, 张静, 高传玉, 等. 急性心肌梗死并发室间隔穿孔患者院内死亡的相关因素分析[J]. 临床心血管病杂志, 2021, 37(12): 1079-1084. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202112003.htm
[5] Figueras J, Alcalde O, Barrabés JA, et al. Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period[J]. Circulation, 2008, 118(25): 2783-2789. doi: 10.1161/CIRCULATIONAHA.108.776690
[6] Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction(2018)[J]. J Am Coll Cardiol, 2018, 72(18): 2231-2264. doi: 10.1016/j.jacc.2018.08.1038
[7] 迪力夏提·吾布力, 田桃, 张兴达, 等. 急性ST段抬高型心肌梗死患者发生心脏破裂的风险预测模型构建及验证[J]. 中国老年学杂志, 2020, 40(3): 449-453. doi: 10.3969/j.issn.1005-9202.2020.03.001
[8] Bates ER. Reperfusion therapy reduces the risk of myocardial rupture complicating ST-elevation myocardial infarction[J]. J Am Heart Assoc, 2014, 3(5): e001368. doi: 10.1161/JAHA.114.001368
[9] 胡嘉禄, 黎音亮, 颜彦, 等. 51例急性心肌梗死(AMI)合并心脏破裂(CR)的临床特征及预后[J]. 复旦学报(医学版), 2015, 42(2): 198-203. doi: 10.3969/j.issn.1672-8467.2015.02.009
[10] Cui H, Ding X, Li W, et al. The neutrophil percentage to albumin ratio as a new predictor of In-Hospital mortality in patients with ST-Segment elevation myocardial infarction[J]. Med Sci Monit, 2019, 25: 7845-7852. doi: 10.12659/MSM.917987
[11] 张芹, 程毅松, 贾禹, 等. 中性粒细胞百分比与白蛋白比值对急性ST段抬高型心肌梗死患者预后的预测价值分析[J]. 临床急诊杂志, 2020, 21(5): 354-358. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202005004.htm
[12] 李伟君, 李应东. 心肌缺血再灌注损伤钙超载及中医药防治策略[J]. 中西医结合心脑血管病杂志, 2013, 11(2): 217-218. doi: 10.3969/j.issn.1672-1349.2013.02.047
[13] 任佳悦, 马骏. 心肌缺血再灌注损伤的研究进展[J]. 心肺血管病杂志, 2019, 38(10): 1074-1076. https://www.cnki.com.cn/Article/CJFDTOTAL-XFXZ201910016.htm
[14] Gulalp B, Karagun O, Tekin A, et al. Cardiac rupture[J]. J Emerg Med, 2013, 44(1): 58-60. doi: 10.1016/j.jemermed.2011.06.128
[15] Honda S, Asaumi Y, Yamane T, et al. Trends in the clinical and pathological characteristics of cardiac rupture in patients with acute myocardial infarction over 35 years[J]. J Am Heart Assoc, 2014, 3(5): e000984. doi: 10.1161/JAHA.114.000984
[16] French JK, Hellkamp AS, Armstrong PW, et al. Mechanical complications after percutaneous coronary intervention in ST-elevation myocardial infarction(from APEX-AMI)[J]. Am J Cardiol, 2010, 105(1): 59-63.
[17] Qian G, Jin RJ, Fu ZH, et al. Development and validation of clinical risk score to predict the cardiac rupture in patients with STEMI[J]. Am J Emerg Med, 2017, 35(4): 589-593. doi: 10.1016/j.ajem.2016.12.033
[18] Fu Y, Li KB, Yang XC. A risk score model for predicting cardiac rupture after acute myocardial infarction[J]. Chin Med J(Engl), 2019, 132(9): 1037-1044.
[19] Gong W, Feng S, Wang X, et al. Beta-blockers reduced the risk of cardiac rupture in patients with acute myocardial infarction: a meta-analysis of randomized control trials[J]. Int J Cardiol, 2017, 232: 171-175. doi: 10.1016/j.ijcard.2017.01.035
[20] Kosuge M, Kimura K, Ishikawa T, et al. Differences between men and women in terms of clinical features of ST-segment elevation acute myocardial infarction[J]. Circ J, 2006, 70(3): 222-226. doi: 10.1253/circj.70.222
[21] Birnbaum Y, Fishbein MC, Blanche C, et al. Ventricular septal rupture after acute myocardial infarction[J]. N Engl J Med, 2002, 347(18): 1426-1432. doi: 10.1056/NEJMra020228
[22] Honda S, Asaumi Y, Yamane T, et al. Trends in the clinical and pathological characteristics of cardiac rupture in patients with acute myocardial infarction over 35 years[J]. J Am Heart Assoc, 2014, 3(5): e000984. doi: 10.1161/JAHA.114.000984
[23] Hao Z, Ma J, Dai J, et al. A real-world analysis of cardiac rupture on incidence, risk factors and in-hospital outcomes in 4190 ST-elevation myocardial infarction patients from 2004 to 2015[J]. Coron Artery Dis, 2020, 31(5): 424-429. doi: 10.1097/MCA.0000000000000877
-
图(2)
表(2)
计量
- 文章访问数: 1144
- PDF下载数: 405
- 施引文献: 0