
The effect of ablation of persistent atrial fibrillation guided by left posterior atrial wall isolation plus special atrial electrograms ablationinlow voltage area
-
摘要: 目的 评价肺静脉隔离基础上,左房后壁电隔离联合电压标测下特殊电位消融指导持续性心房颤动(房颤)消融的疗效。方法 入选221例首次接受房颤射频消融治疗的持续性房颤患者,其中对照组(101例)行单纯肺静脉隔离,研究组(120例)在肺静脉隔离基础上,首先行Box消融,验证后壁电隔离情况并补点消融,根据电压标测结果在低电压区及移行区标测、标记及消融特殊电位。分析两组术中消融数据及术后患者长期随访结果等。结果 平均随访(22.3±6.9)个月,对照组患者成功率为49.5%,研究组首次手术后成功率约为69.2%,Kaplan-Meier法分析提示两组首次术后成功率有统计学差异(P=0.006 2)。结论 持续性房颤患者接受左房后壁电隔离联合电压标测指导特殊电位消融安全有效。Abstract: Objective To evaluate the efficacy of ablation of persistent atrial fibrillation guided by the left atrial posterior wall electrical isolation combined with voltage mapping to guide the special potential ablation on the basis of pulmonary vein isolation.Methods A total of 221 patients with persistent atrial fibrillation who received radiofrequency ablation of atrial fibrillation for the first time were selected. The control group underwent simple pulmonary vein isolation(101 patients), and the study group(120 patients) underwent Box ablation based on pulmonary vein isolation. The electrical isolation of the wall and the point of ablation are added in them. According to the voltage mapping results, special potentials are mapped, marked and ablated in the low-voltage area and the transition area. The intraoperative ablation data and postoperative long-term follow-up results of the two groups were analyzed.Results The time of average follow-up was(22.3±6.9) months. The success rate after the first operation in the control group was 49.5%, and the success rate in the research group was about 69.2%(P=0.006 2).Conclusion The left atrial posterior wall electrical isolation combined with voltage mapping to guide the special potential ablation in patients with persistent atrial fibrillation is safe and effective.
-
Key words:
- atrial fibrillation /
- catheter ablation /
- efficacy
-

-
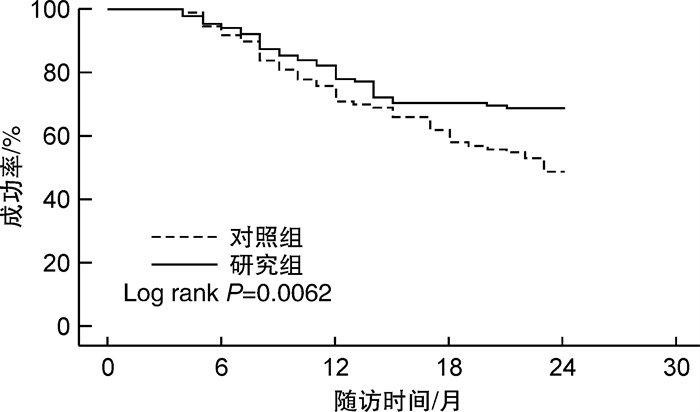
图 1 首次术后两组成功率对比
Figure 1. Kaplan-Meier survival curves for the freedom from atrial tachyarrhythmias after ablation
表 1 两组患者基线资料比较
Table 1. Baseline data
例(%), X±S 项目 研究组(120例) 对照组(101例) P值 年龄/岁 59.4±10.6 57.3±10.3 0.200 男 76(63.3) 69(68.3) 0.437 BMI/(kg·m-2) 25.6±2.5 26.1±1.8 0.176 冠心病 10(8.3) 7(6.9) 0.697 高血压 62(51.7) 54(53.5) 0.790 心衰 3(2.5) 2(2.0) 0.796 左房内径/mm 46.4±3.6 45.8±3.9 0.498 左室射血分数/% 59.1±5.4 60.1±5.8 0.101 左房低电压区及占比 前壁 101(84.2) 84(83.2) 0.841 后壁 53(44.2) 50(49.5) 0.428 顶部 59(49.2) 52(51.5) 0.731 间隔 47(39.2) 43(42.6) 0.608 底部 38(31.7) 39(38.6) 0.280 低电压区/左房面积/% 31.2±8.9 30.5±9.7 0.547  下载: 导出CSV
下载: 导出CSV
表 2 首次术后两组复发心律失常类型比较
Table 2. Comparison of types of recurrent arrhythmias after operation
例(%) 复发类型 研究组(120例) 对照组(101例) P值 阵发性房颤 21(17.5) 8(7.9) 0.036 持续性房颤 6(5.0) 37(36.6) < 0.010 房速 10(8.3) 6(5.9) 0.494
下载: 导出CSV
-
[1] Pak HN, Hwang C, Lim HE, et al. Electroanatomic characteristics of atrial premature beats triggering atrial fibrillation in patients with persistent versus paroxysmal atrial fibrillation[J]. J Cardiovasc Electrophysiol, 2006, 17(8): 818-824. doi: 10.1111/j.1540-8167.2006.00503.x
[2] Verma A, Jiang CY, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation[J]. N Engl J Med, 2015, 372(19): 1812-1822. doi: 10.1056/NEJMoa1408288
[3] 彭飞, 连晓雨, 张和细, 等. 肺静脉前庭放射状线性消融改良术式治疗持续性房颤——临床Pilot研究[J]. 临床心血管病杂志, 2021, 37(9): 801-804. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202109005.htm
[4] Thiyagarajah A, Kadhim K, Lau DH, et al. Feasibility, safety, and efficacy of posterior wall isolation during atrial fibrillation ablation: a systematic review and meta-analysis[J]. Circ Arrhythm Electrophysiol, 2019, 12(8): e007005. doi: 10.1161/CIRCEP.118.007005
[5] Jadidi AS, Lehrmann H, Keyl C, et al. Ablation of persistent atrial fibrillation targeting low-voltage areas with selective activation characteristics[J]. Circ Arrhy Electrophysiol, 2016, 9(3): e002962. doi: 10.1161/CIRCEP.115.002962
[6] Pan Q, Xu WJ, Tang YQ, et al. Unique histological features of the left atrial posterior wall[J]. J Int Med Res, 2009, 37(2): 392-399. doi: 10.1177/147323000903700214
[7] 胡润晖, 胡建平, 洪葵. 自主神经与心房颤动的研究进展[J]. 临床心血管病杂志, 2020, 36(1): 86-89. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202001020.htm
[8] Wu TJ, Doshi RN, Huang HL, et al. Simultaneous biatrial computerized mapping during permanent atrial fibrillation in patients with organic heart disease[J]. J Cardiovasc Electrophysiol, 2002, 13(6): 571-577. doi: 10.1046/j.1540-8167.2002.00571.x
[9] Elayi CS, Di Biase L, Bai R, et al. Administration of isoproterenol and adenosine to guide supplemental ablation after pulmonary vein antrum isolation[J]. J Cardiovasc Electrophysiol, 2013, 24(11): 1199-1206. doi: 10.1111/jce.12252
[10] Corradi D, Callegari S, Gelsomino S, et al. Morphology and pathophysiology of target anatomical sites for ablation procedures in patients with atrial fibrillation: part Ⅱ: pulmonary veins, caval veins, ganglionated plexi, and ligament of Marshall[J]. Int J Cardiol, 2013, 168(3): 1769-1778. doi: 10.1016/j.ijcard.2013.06.141
[11] Lee AM, Aziz A, Didesch J, et al. Importance of atrial surface area and refractory period in sustaining atrial fibrillation: testing the critical mass hypothesis[J]. J Thorac Cardiovasc Surg, 2013, 146(3): 593-598. doi: 10.1016/j.jtcvs.2012.04.021
[12] Jadidi AS, Cochet H, Shah AJ, et al. Inverse relationship between fractionated electrograms and atrial fibrosis in persistent atrial fibrillation: combined magnetic resonance imaging and high-density mapping[J]. J Am Coll Cardiol, 2013, 62(9): 802-812. doi: 10.1016/j.jacc.2013.03.081
[13] Harrison JL, Jensen HK, Peel SA, et al. Cardiac magnetic resonance and electroanatomical mapping of acute and chronic atrial ablation injury: a histological validation study[J]. Eur Heart J, 2014, 35(22): 1486-1495. doi: 10.1093/eurheartj/eht560
[14] Haissaguerre M, Shah AJ, Cochet H, et al. Intermittent drivers anchoring to structural heterogeneities as a major pathophysiological mechanism of human persistent atrial fibrillation[J]. J Physiol, 2016, 594(9): 2387-2398. doi: 10.1113/JP270617
[15] Yagishita A, Gimbel JR, DE Oliveira S, et al. Long-term outcome of left atrial voltage-guided substrate ablation during atrial fibrillation: a novel adjunctive ablation strategy[J]. J Cardiovasc Electrophysiol, 2017, 28(2): 147-155. doi: 10.1111/jce.13122
[16] Takahashi Y, O'Neill MD, Hocini M, et al. Characterization of electrograms associated with termination of chronic atrial fibrillation by catheter ablation[J]. J Am Coll Cardiol, 2008, 51(10): 1003-1010. doi: 10.1016/j.jacc.2007.10.056
[17] Della Rocca DG, Mohanty S, Mohanty P, et al. Long-term outcomes of catheter ablation in patients with longstanding persistent atrial fibrillation lasting less than 2 years[J]. J Cardiovasc Electrophysiol, 2018, 29(12): 1607-1615. doi: 10.1111/jce.13721
-
图(1)
表(2)
计量
- 文章访问数: 2082
- PDF下载数: 1656
- 施引文献: 0