
-
摘要: 癌症是全世界死亡的主要原因之一,不断演进的抗癌药物使癌症患者的生存期明显延长。心血管疾病逐步取代癌症本身成为癌症患者致死和致残的主要原因,高血压是其中最常见的心血管疾病之一,所以监测及管理肿瘤患者的血压对降低化疗引起的心脏毒性风险和降低长期心血管疾病的风险至关重要。本文主要回顾与高血压发生相关的常见抗肿瘤药物,包括血管内皮生长因子抑制剂、小分子酪氨酸激酶抑制剂、蛋白酶体抑制剂、烷基化剂和免疫抑制剂等相关高血压的流行病学、潜在机制及针对性的管理建议,并讨论癌症患者应用血管内皮生长因子信号通路抑制剂相关血压的评估和管理策略。Abstract: Cancer is one of the leading causes of death worldwide, and the evolution of anti-cancer drugs has significantly prolonged the life expectancy of cancer patients. Cardiovascular diseases have gradually replaced cancer as the leading cause of morbidity and mortality in cancer patients. Among these cancer patients, hypertension is one of the most common cardiovascular diseases. Therefore, monitoring and managing blood pressure in cancer patients is crucial to reducing the risk of cardiotoxicity caused by chemotherapy and the risk of cardiovascular diseases. In this review, we reviewed common antitumor drugs related to hypertension, including vascular endothelial growth factor (VEGF) inhibitors, small molecule tyrosine kinase inhibitors, protease inhibitors, alkylating agents, and immunosuppressants. We also discussed epidemiology, underlying mechanisms, and corresponding management advice of these antitumor drugs. Finally, we discussed the blood pressure assessment and management strategy for cancer patients using VEGF pathway inhibitors.
-
Key words:
- hypertension /
- cardio-oncology /
- cardiotoxicity
-

-
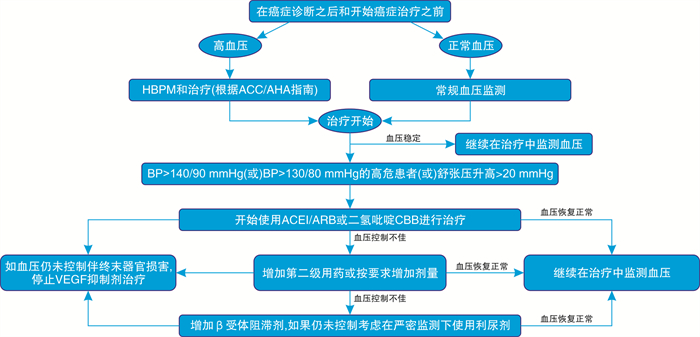
图 1 VEGF信号通路抑制剂相关高血压的管理方法
Figure 1. Management of VEGF signaling pathway inhibitor related hypertension
表 1 抗肿瘤药物相关高血压的发生率、机制及管理
Table 1. Incidence rate, mechanism and management of anti-tumor drug-related hypertension
药物种类 机制 高血压发生率/% 治疗 VEGF抑制剂 内皮功能障碍,抑制NO途径(NO和前列环素I减少),内皮素-1增加,血管重塑,全身血栓性微血管病和氧化应激,毛细血管稀疏,肾钠排泄减少 17~80 CCB(如氨氯地平)、ACEI(如赖诺普利) 酪氨酸激酶抑制剂 NOS活性降低,RAAS激活 17~47 ACEI或CCB 蛋白酶体抑制剂 血管紧张素诱导高血压,主动脉血管重构,血栓性微血管病 3~15 ACEI或ARB(如氯沙坦) 烷化剂 内皮细胞氧化损伤、内膜厚度增加,血管重塑异常,钠潴留、肾毒性和微量白蛋白血症 36~50 ACEI或ARB 钙调神经磷酸酶抑制剂和其他免疫抑制剂 交感神经过度活动,肾动脉血管收缩,肾钠重吸收增加、纳潴留(远端小管上皮钠通道激活),NO生成减少,RAAS激活,肾前列腺素合成改变 30~80 CCB、噻嗪类利尿剂(尤其是他克莫司) 阿比特龙 具有盐皮质激素特性的类固醇前体增加(钠和液体滞留) 盐皮质激素拮抗剂、利尿剂 紫杉烷 内皮功能障碍、贝伐单抗和蒽环类药物毒性增强 ACEI、ARB或CCB  下载: 导出CSV
下载: 导出CSV
-
[1] Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020[J]. CA Cancer J Clin, 2020, 70(1): 7-30. doi: 10.3322/caac.21590
[2] Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health conditions in adult survivors of childhood cancer[J]. N Engl J Med, 2006, 355(15): 1572-1582. doi: 10.1056/NEJMsa060185
[3] Lenihan DJ, Cardinale D, Cipolla CM. The compelling need for a cardiology and oncology partnership and the birth of the International Cardi-Oncology Society[J]. Prog Cardiovasc Dis, 2010, 53(2): 88-93. doi: 10.1016/j.pcad.2010.06.002
[4] Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer[J]. N Engl J Med, 2015, 372(7): 621-630. doi: 10.1056/NEJMoa1406470
[5] Fuchs FD, Whelton PK. High Blood Pressure and Cardiovascular Disease[J]. Hypertension, 2020, 75(2): 285-292. doi: 10.1161/HYPERTENSIONAHA.119.14240
[6] Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension[J]. J Hypertension. 2018, 36(10): 1953-2041. doi: 10.1097/HJH.0000000000001940
[7] Souza VB, Silva EN, Ribeiro ML, et al. Hypertension in patients with cancer[J]. Arq Bras Cardiol, 2015, 104(3): 246-252.
[8] Hein TW, Rosa RH Jr, Ren Y, et al. VEGF Receptor-2-Linked PI3K/Calpain/SIRT1 Activation Mediates Retinal Arteriolar Dilations to VEGF and Shear Stress[J]. Invest Ophthalmol Vis Sci, 2015, 56(9): 5381-5389. doi: 10.1167/iovs15-16950
[9] Viallard C, Larrivée B. Tumor angiogenesis and vascular normalization: alternative therapeutic targets[J]. Angiogenesis, 2017, 20(4): 409-426. doi: 10.1007/s10456-017-9562-9
[10] Simons M, Gordon E, Claesson-Welsh L. Mechanisms and regulation of endothelial VEGF receptor signalling[J]. Nat Rev Mol Cell Biol, 2016, 17(10): 611-625.
[11] Kamli H, Li L, Gobe GC. Limitations to the Therapeutic Potential of Tyrosine Kinase Inhibitors and Alternative Therapies for Kidney Cancer[J]. Ochsner J, 2019, 19(2): 138-151. doi: 10.31486/toj.18.0015
[12] Small HY, Montezano AC, Rios FJ, et al. Hypertension due to antiangiogenic cancer therapy with vascular endothelial growth factor inhibitors: understanding and managing a new syndrome[J]. Can J Cardiol, 2014, 30(5): 534-543. doi: 10.1016/j.cjca.2014.02.011
[13] Syrigos KN, Karapanagiotou E, Boura P, et al. Bevacizumab-induced hypertension: pathogenesis and management[J]. BioDrugs, 2011, 25(3): 159-169. doi: 10.2165/11590180-000000000-00000
[14] Versmissen J, Mirabito Colafella KM, Koolen S, et al. Vascular Cardio-Oncology: Vascular Endothelial Growth Factor inhibitors and hypertension[J]. Cardiovasc Res, 2019, 115(5): 904-914. doi: 10.1093/cvr/cvz022
[15] Gressett SM, Shah SR. Intricacies of bevacizumab-induced toxicities and their management[J]. Ann Pharmacother, 2009, 43(3): 490-501. doi: 10.1345/aph.1L426
[16] Li M, Kroetz DL. Bevacizumab-induced hypertension: Clinical presentation and molecular understanding[J]. Pharmacol Ther, 2018, 182: 152-160. doi: 10.1016/j.pharmthera.2017.08.012
[17] Frey MK, Dao F, Olvera N, et al. Genetic predisposition to bevacizumab-induced hypertension[J]. Gynecol Oncol, 2017, 147(3): 621-625. doi: 10.1016/j.ygyno.2017.09.017
[18] Valent P, Hadzijusufovic E, Hoermann G, et al. Risk factors and mechanisms contributing to TKI-induced vascular events in patients with CML[J]. Leuk Res, 2017, 59: 47-54. doi: 10.1016/j.leukres.2017.05.008
[19] Plummer C, Michael A, Shaikh G, et al. Expert recommendations on the management of hypertension in patients with ovarian and cervical cancer receiving bevacizumab in the UK[J]. Br J Cancer, 2019, 121(2): 109-116. doi: 10.1038/s41416-019-0481-y
[20] Touyz RM, Herrmann J. Cardiotoxicity with vascular endothelial growth factor inhibitor therapy[J]. NPJ Precis Oncol, 2018, 2: 13.
[21] Izzedine H, Ederhy S, Goldwasser F, et al. Management of hypertension in angiogenesis inhibitor-treated patients[J]. Ann Oncol, 2009, 20(5): 807-815. doi: 10.1093/annonc/mdn713
[22] Souza VB, Silva EN, Ribeiro ML, et al. Hypertension in patients with cancer[J]. Arq Bras Cardiol, 2015, 104(3): 246-252.
[23] Corr BR, Breed C, Sheeder J, et al. Bevacizumab induced hypertension in gynecologic cancer: Does it resolve after completion of therapy?[J]. Gynecol Oncol Rep, 2016, 17: 65-68. doi: 10.1016/j.gore.2016.06.002
[24] Li Y, Li S, Zhu Y, et al. Incidence and risk of sorafenib-induced hypertension: a systematic review and meta-analysis[J]. J Clin Hypertens(Greenwich), 2014, 16(3): 177-185. doi: 10.1111/jch.12273
[25] Fu Y, Wei X, Lin L, et al. Adverse reactions of sorafenib, sunitinib, and imatinib in treating digestive system tumors[J]. Thorac Cancer, 2018, 9(5): 542-547. doi: 10.1111/1759-7714.12608
[26] Kollmannsberger C, Soulieres D, Wong R, et al. Sunitinib therapy for metastatic renal cell carcinoma: recommendations for management of side effects[J]. Can Urol Assoc J, 2007, 1(2 Suppl): S41-54.
[27] Hasinoff BB, Patel D, Wu X. Molecular Mechanisms of the Cardiotoxicity of the Proteasomal-Targeted Drugs Bortezomib and Carfilzomib[J]. Cardiovasc Toxicol, 2017, 17(3): 237-250.
[28] Chari A, Hajje D. Case series discussion of cardiac and vascular events following carfilzomib treatment: possible mechanism, screening, and monitoring[J]. BMC Cancer, 2014, 14: 915.
[29] Wu P, Oren O, Gertz MA, et al. Proteasome Inhibitor-Related Cardiotoxicity: Mechanisms, Diagnosis, and Management[J]. Curr Oncol Rep, 2020, 22(7): 66.
[30] Cameron AC, Touyz RM, Lang NN. Vascular Complications of Cancer Chemotherapy[J]. Can J Cardiol, 2016, 32(7): 852-862.
[31] Kooijmans EC, Bökenkamp A, Tjahjadi NS, et al. Early and late adverse renal effects after potentially nephrotoxic treatment for childhood cancer[J]. Cochrane Database Syst Rev, 2019, 3: CD008944.
[32] Soultati A, Mountzios G, Avgerinou C, et al. Endothelial vascular toxicity from chemotherapeutic agents: preclinical evidence and clinical implications[J]. Cancer Treat Rev, 2012, 38(5): 473-483.
[33] Morales JM. Influence of the new immunosuppressive combinations on arterial hypertension after renal transplantation[J]. Kidney Int Suppl, 2002, (82): S81-S87.
[34] Haddad EM, McAlister VC, Renouf E, et al. Cyclosporin versus tacrolimus for liver transplanted patients[J]. Cochrane Database Syst Rev, 2006, (4): CD005161.
[35] Zhai YJ, Wu MM, Linck VA, et al. Intracellular cholesterol stimulates ENaC by interacting with phosphatidylinositol-4, 5-bisphosphate and mediates cyclosporine A-induced hypertension[J]. Biochim Biophys Acta Mol Basis Dis, 2019, 1865(7): 1915-1924.
[36] Divac N, Naumović R, Stojanović R, et al. The Role of Immunosuppressive Medications in the Pathogenesis of Hypertension and Efficacy and Safety of Antihypertensive Agents in Kidney Transplant Recipients[J]. Curr Med Chem, 2016, 23(19): 1941-1952.
[37] Chanard J, Toupance O, Lavaud S, et al. Amlodipine reduces cyclosporin-induced hyperuricaemia in hypertensive renal transplant recipients[J]. Nephrol Dial Transplant, 2003, 18(10): 2147-2153.
[38] Vergoulas G. Antihypertensive agents and renal transplantation[J]. Hippokratia, 2007, 11(1): 3-12.
[39] Lazelle RA, McCully BH, Terker AS, et al. Renal Deletion of 12 kDa FK506-Binding Protein Attenuates Tacrolimus-Induced Hypertension[J]. J Am Soc Nephrol, 2016, 27(5): 1456-1464.
[40] Vasaitis TS, Bruno RD, Njar VC. CYP17 inhibitors for prostate cancer therapy[J]. J Steroid Biochem Mol Biol, 2011, 125(1-2): 23-31.
[41] Veccia A, Maines F, Kinspergher S, et al. Cardiovascular toxicities of systemic treatments of prostate cancer[J]. Nat Rev Urol, 2017, 14(4): 230-243.
[42] Canela MD, Noppen S, Bueno O, et al. Antivascular and antitumor properties of the tubulin-binding chalcone TUB091[J]. Oncotarget, 2017, 8(9): 14325-14342.
[43] Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Hypertensio, 2018, 71(6): 1269-1324.
[44] Gressett SM, Shah SR. Intricacies of bevacizumab-induced toxicities and their management[J]. Ann Pharmacother, 2009, 43(3): 490-501.
[45] Menditto E, Gimeno Miguel A, Moreno Juste A, et al. Patterns of multimorbidity and polypharmacy in young and adult population: Systematic associations among chronic diseases and drugs using factor analysis[J]. PLoS One, 2019, 14(2): e0210701.
[46] MacDonald TM, Williams B, Webb DJ, et al. Combination Therapy Is Superior to Sequential Monotherapy for the Initial Treatment of Hypertension: A Double-Blind Randomized Controlled Trial[J]. J Am Heart Assoc, 2017, 6(11).
[47] Humphreys BD, Atkins MB. Rapid development of hypertension by sorafenib: toxicity or target?[J]. Clin Cancer Res, 2009, 15(19): 5947-5949.
[48] Jain M, Townsend RR. Chemotherapy agents and hypertension: a focus on angiogenesis blockade[J]. Curr Hypertens Rep, 2007, 9(4): 320-328.
-
图(1)
表(1)
计量
- 文章访问数: 3080
- PDF下载数: 1904
- 施引文献: 0