
The relationship between body mass index and the late recurrence of atrial fibrillation after ablation
-
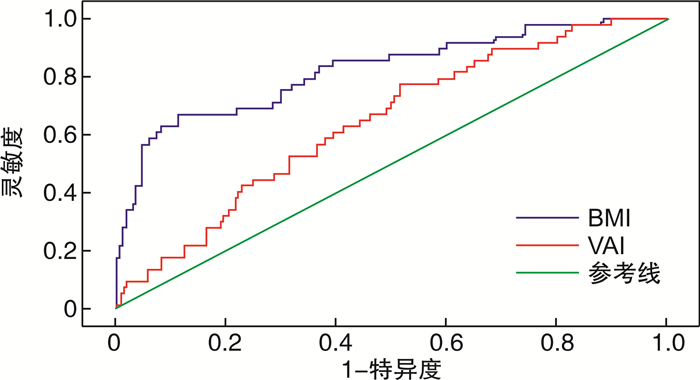
摘要: 目的分析体质量指数(BMI)及肥胖相关指标与心房颤动(房颤)消融术后复发的关系。方法回顾性分析2015年1月1日—2021年6月30日因阵发性房颤且行导管消融术的319例患者,根据房颤消融术后是否复发分为复发组(91例)、未复发组(228例),根据复发时间将复发患者分为晚期复发组49例、极晚期复发组42例,分析各组肥胖指标差异、临床特点;采用Cox回归分析探索房颤复发组及晚期复发组的危险因素;采用受试者工作特征曲线(ROC曲线)分析肥胖指标预测房颤复发的价值。结果① 复发组的BMI高于未复发组[(26.70±2.69) kg/m2:(24.38±2.17) kg/m2],复发组的腰围(WC)、腰高比(WHtR)、脂质蓄积指数(LAP)、内脏肥胖指数(VAI)、心脏代谢指数(CMI)、体脂指数(BAI)等肥胖指标也高于未复发组(均P < 0.05)。②晚期复发组的BMI[(27.68±2.50) kg/m2:(25.56±2.47) kg/m2]、WHR、VAI高于极晚期复发组(均P < 0.05)。③多因素Cox回归分析显示,晚期复发(1年内复发)的独立预测因素是:BMI、VAI、白细胞计数、肌钙蛋白T(均P < 0.05);极晚期复发(1年后复发)独立预测因素是:冠心病、中性粒细胞计数、空腹血糖(均P < 0.05)。④ROC曲线分析显示,BMI预测房颤消融术后1年内复发的价值(AUC=0.822,P=0.036,95%CI:0.752~0.892)高于VAI(AUC=0.645,P=0.001,95%CI:0.567~0.723)。结论BMI是预测房颤消融术后晚期复发的肥胖指标。Abstract: ObjectiveTo analyze the relationship between obesity-related indexes and recurrence after atrial fibrillation ablation.MethodsThe 319 patients who underwent catheter ablation for paroxysmal atrial fibrillation were included. According to the recurrence of atrial fibrillation after ablation, they were divided into recurrence group(91 cases) and non-recurrence group(228 cases). According to whether the postoperative recurrence time was within 1 year, the recurrent patients were divided into late recurrence group(49 cases) and very late recurrence group(42 cases). Cox regression analysis was used to explore the risk factors of recurrence group, late recurrence of atrial fibrillation group and very late recurrence group. Then, the receiver-operating characteristic curve analysis was used to analyze the value of obesity index to predict the recurrence of atrial fibrillation.Results⑴BMI of recurrent group was higher than that of non-recurrent group[(26.70±2.69) kg/m2vs(24.38±2.17) kg/m2], waist circumstance(WC), waist-to-hip ratio(WHtR), lipid Accumulation Product(LAP), visceral obesity index(VAI), cardiometabolic Index(CMI), body fat index(BAI) and other obesity indexes were also higher than those of the non-recurrent group(all P < 0.05); ⑵BMI of late recurrence group was higher than that of very late recurrence group[(27.68±2.50) kg/m2vs(25.56±2.47) kg/m2], WHR, VAI were also higher than those of the very late recurrence group(all P < 0.05); ⑶Multiple Cox regression analysis showed that the independent predictors of late recurrence(recurrence within one year) were BMI(HR: 1.269, 95%CI: 1.131-1.423), VAI(HR: 1.004, 95%CI: 1.001-1.007) and white blood cell count(HR: 1.232, 95%CI: 1.032-1.470). The independent predictors of very late recurrence(recurrence after 1 year) were coronary heart disease, neutrophil count and fasting blood glucose(all P < 0.05); ⑷ROC curve analysis showed that the value of BMI in predicting recurrence of atrial fibrillation within one year after ablation(AUC=0.822, P=0.036, 95%CI: 0.752-0.892) was higher than of VAI(AUC=0.645, P=0.001, 95%CI: 0.567-0.792).ConclusionBMI is the obesity index to predict late recurrence of atrial fibrillation after ablation.
-
Key words:
- obesity /
- atrial fibrillation /
- catheter ablation /
- body mass index
-

-
表 1 复发组与未复发组基线资料比较
Table 1. General data
例(%), X±S, M(P25, P75) 项目 未复发组(228例) 复发组(91例) P值 年龄/岁 62(54,67) 61(54,68) 0.853 男性 153(67.11) 52(57.14) 0.094 既往病史 高血压史 106(46.49) 41(45.05) 0.816 冠心病史 48(21.05) 19(20.88) 0.973 糖尿病史 32(14.04) 14(15.38) 0.757 吸烟史 82(35.96) 31(34.07) 0.749 饮酒史 46(20.18) 17(18.68) 0.795 房颤持续时间/月 7(1,24) 12(2,36) 0.117 收缩压/mmHg△ 121.84±16.29 126.45±17.82 0.027 舒张压/mmHg 78(70,85) 78(70,82) 0.331 心率/(次·min-1) 77.71±17.51 74.26±12.38 0.049 手术方式 0.953 冷冻消融 86(37.72) 34(37.36) 射频消融 142(62.28) 57(62.64) 肥胖指标 WC/cm 90.50(85.00,96.00) 93.00(89.00,100.00) 0.001 WHR 0.91±0.05 0.92±0.06 0.191 WHtR 0.53(0.51,0.57) 0.56(0.54,0.58) < 0.001 VAI 106.47(81.08,143.29) 114.19(94.22,163.79) 0.023 LAP 29.06(21.09,41.69) 34.88(26.25,54.80) 0.003 CMI 0.59(0.39,0.86) 0.61(0.46,0.96) 0.022 BMI/(kg·m-2) 24.38±2.17 26.70±2.69 < 0.001 BAI 27.69±3.31 29.23±3.78 < 0.001 心脏超声 左房内径/mm 35(32,38) 36(32,40) 0.038 左室收缩末内径/mm 30(28,33) 32(29,35) 0.026 左室舒张末内径/mm 49(47,52) 50(47,52) 0.062 左室射血分数/% 67(62,71) 65(62,69) 0.159 注:△1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 晚期复发和极晚期复发组间基线资料比较
Table 2. Data in LR group and VLR group
例(%), X±S, M(P25, P75) 项目 晚期复发组(49例) 极晚期复发组(42例) P值 年龄/岁 60.84±9.29 60.64±9.79 0.923 男性 34(69.39) 18(42.86) 0.011 既往病史 高血压史 24(48.98) 17(40.48) 0.416 冠心病史 13(26.53) 6(14.29) 0.152 糖尿病史 7(14.29) 7(16.67) 0.905 吸烟史 21(42.86) 10(23.81) 0.056 饮酒史 9(18.37) 8(19.05) 0.971 房颤持续时间/月 12.00(1.00,42.00) 15.00(2.75,36.00) 0.451 收缩压/mmHg 126.47±18.82 126.43±16.81 0.991 舒张压/mmHg 77.86±10.35 75.50±8.21 0.237 心率/(次·min-1) 75.31±14.59 73.05±9.19 0.389 CHA2DS2-VASc/分 2(1,3) 2(1,3) 0.416 Hasbled/分 1(0,1) 1(0,2) 0.567 手术方式 0.762 冷冻消融 20(40.82) 14(33.33) 射频消融 29(59.18) 28(66.67) 肥胖指标 WC/cm 95.00(90.00,101.00) 92(87.00,97.25) 0.061 WHR 0.94±0.05 0.90±0.06 0.004 WHtR 0.57±0.04 0.55±0.04 0.079 VAI 126.60(105.05,176.39) 110.46(85.04,135.94) 0.021 LAP 41.50(25.86,59.43) 33.28(26.20,41.85) 0.184 CMI 0.68(0.46,1.05) 0.54(0.45,0.93) 0.255 BMI/(kg·m-2) 27.68±2.50 25.56±2.47 0.000 BAI 28.93±4.13 29.58±3.33 0.412 实验室检查 LDL-C/(mmol·L-1) 2.23±0.89 1.88±0.62 0.038 脂蛋白a/(mg·L-1) 82.70(24.80,208.10) 139.00(73.75,311.25) 0.020 空腹血糖/(mmol·L-1) 5.21(4.59,6.12) 5.18(4.66,6.10) 0.238 糖化血红蛋白/% 5.80(5.55,6.25) 5.70(5.38,6.00) 0.515 NT-proBNP/(pg·mL-1) 410.00(88.80,881.8) 220.65(122.03,454.10) 0.331 肌钙蛋白T/(ng·mL-1) 0.008(0.006,0.017) 0.006(0.004,0.008) 0.001 尿素氮/(mmol·L-1) 5.76±1.95 5.83±1.64 0.864 肌酐/(μmol·L-1) 71.88±18.12 64.07±14.41 0.027 胱抑素C/(mg·L-1) 0.98±0.36 0.80±0.28 0.011 尿酸/(μmol·L-1) 330.98±93.67 294.56±52.86 0.028 红细胞计数/(×1012·L-1) 4.70±0.52 4.43±0.62 0.022 血小板计数/(×109·L-1) 174.50(131.75,218.75) 173.00(116.00,220.00) 0.012 白细胞计数/(×109·L-1) 5.94±1.59 6.13±1.67 0.051 中性粒细胞/(×109·L-1) 4.31±1.47 3.71±1.44 0.052 心脏超声 左房内径/mm 36(32,40) 35.5(32,40) 0.663 左室收缩末内径/mm 32(30,35) 31(29,33) 0.086 左室舒张末内径/mm 51(48,54) 49(47,52) 0.032 左室射血分数/% 65(61,69) 66(63,70) 0.425 注:CHA2DS2-VASc:房颤卒中风险评分;Hasbled:房颤出血风险评分;NT-proBNP:N末端-B型脑尿钠肽前体。
下载: 导出CSV
表 3 房颤消融术后晚期复发的多因素Cox回归分析
Table 3. Multiariable Cox regression analysis
变量 多因素Cox回归分析 HR 95%CI P值 BMI 1.269 1.131~1.423 0.000 VAI 1.004 1.001~1.007 0.011 白细胞计数 1.232 1.032~1.470 0.021 肌钙蛋白T 1.709 1.031~2.883 0.038
下载: 导出CSV
表 4 房颤消融术后极晚期复发的多因素Cox回归分析
Table 4. Multiariable Cox regression analysis
变量 多因素Cox回归分析 HR 95%CI P值 冠心病史1) 3.168 1.180~8.508 0.022 中性粒细胞计数 1.476 1.125~1.935 0.005 空腹血糖 1.375 0.972~1.946 0.009 注:1)冠心病史赋值:0=无,1=有,以最小的赋值作为参考。
下载: 导出CSV
-
[1] Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The Evidence Report(1998) National Institutes of Health[J]. Obes Res, 1998, 6 Suppl 2: 899-917.
[2] 林秋珍, 韩冰, 刘启明. 心房颤动诊断管理指南更新解读[J]. 临床心血管病杂志, 2021, 37(5): 485-488. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202105018.htm
[3] Bergman RN, Stefanovski D, Buchanan TA, et al. A better index of body adiposity[J]. Obesity, 2011, 19: 1083e9.
[4] World Health Organization. Waist circumference and waist-hip ratio: report of a WHO expert consultation, Geneva, 8-11 December 2008[R]. Geneva: World Health Organization, 2011: 27.
[5] Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value[J]. Nutr Res Rev, 2010, 23(2): 247-269. doi: 10.1017/S0954422410000144
[6] Amato MC, Giordano C, Galia M, et al. Visceral adiposity index: a reliable indicator of visceral fat function associated with cardiometabolic risk[J]. Diabetes Care, 2010, 33(4): 920-922. doi: 10.2337/dc09-1825
[7] Kahn HS. The "lipid accumulation product" performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison[J]. BMC Cardiovasc Disord, 2005, 5: 26. doi: 10.1186/1471-2261-5-26
[8] Wakabayashi I, Daimon T. The"cardiometabolic index"as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus[J]. Clin Chim Acta, 2015, 438: 274-278. doi: 10.1016/j.cca.2014.08.042
[9] 廖玉华, 余淼, 史河水. 心外膜脂肪组织: 心血管病防治的新靶点[J]. 临床心血管病杂志, 2020, 36(1): 11-14. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202001002.htm
[10] 李雪博, 李昌海, 王孝锋. 心外膜脂肪组织、肥胖与心房颤动[J]. 研究进展, 2020, 36(2): 193-195. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202002022.htm
[11] Tedrow UB, Conen D, Ridker PM, et al. The long-and short-term impact of elevated body mass index on the risk of new atrial fibrillation the WHS(women's health study)[J]. J Am Coll Cardiol, 2010, 55(21): 2319-2327. doi: 10.1016/j.jacc.2010.02.029
[12] Conen D, Tedrow UB, Koplan BA, et al. Influence of systolic and diastolic blood pressure on the risk of incident atrial fibrillation in women[J]. Circulation, 2009, 119(16): 2146-2152. doi: 10.1161/CIRCULATIONAHA.108.830042
[13] Sivasambu B, Balouch MA, Zghaib T, et al. Increased rates of atrial fibrillation recurrence following pulmonary vein isolation in overweight and obese patients[J]. J Cardiovasc Electrophysiol, 2018, 29(2): 239-245. doi: 10.1111/jce.13388
[14] Deng H, Shantsila A, Guo P, et al. A U-shaped relationship of body mass index on atrial fibrillation recurrence post ablation: A report from the Guangzhou atrial fibrillation ablation registry[J]. EBioMedicine, 2018, 35: 40-45. doi: 10.1016/j.ebiom.2018.08.034
[15] Glover BM, Hong KL, Dagres N, et al. Impact of body mass index on the outcome of catheter ablation of atrial fibrillation[J]. Heart, 2019, 105(3): 244-250. doi: 10.1136/heartjnl-2018-313490
[16] Zethof M, Mosterd CM, Collard D, et al. Differences in body composition convey a similar risk of type 2 diabetes among different ethnic groups with disparate cardiometabolic risk-the HELIUS Study[J]. Diabetes Care, 2021, 44(7): 1692-1698. doi: 10.2337/dc21-0230
[17] Streng KW, Voors AA, Hillege HL, et al. Waist-to-hip ratio and mortality in heart failure[J]. Eur J Heart Fail, 2018, 20(9): 1269-1277. doi: 10.1002/ejhf.1244
[18] Houghton SC, Eliassen H, Tamimi RM, et al. Central adiposity and subsequent risk of breast cancer by menopause status[J]. J Natl Cancer Inst, 2021, 113(7): 900-908. doi: 10.1093/jnci/djaa197
-
图(1)
表(4)
计量
- 文章访问数: 2277
- PDF下载数: 805
- 施引文献: 0