
-
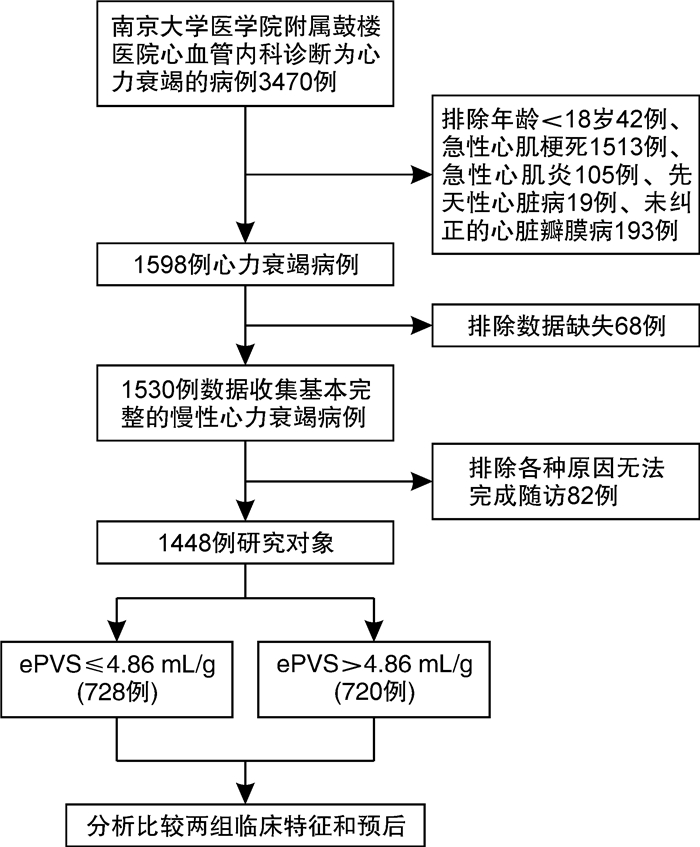
摘要: 目的评估血浆容量状态对心力衰竭(心衰)患者预后的影响。方法选择2010年9月—2019年5月在南京大学医学院附属鼓楼医院心血管内科住院并以心衰为主要诊断的患者1448例,使用Duarte公式根据血红蛋白和红细胞压积计算得出估测血浆容量状态(ePVS)结果,根据中位数分为ePVS低值组和高值组,比较两组基本临床特征,通过生存分析比较两组1年、5年的心血管死亡和主要不良心血管事件发生率,评估ePVS对心衰患者预后的影响。结果ePVS低值组和高值组心血管死亡率1年和5年均有统计学差异(3.4% vs 8.3%,P < 0.001;8.4% vs 16.5%,P < 0.001),ePVS高值组1年和5年的主要心血管不良事件发生率均高于低值组(37.1% vs 29.8%,P=0.004;66.4% vs 54.8%,P < 0.001)。经过多因素Cox回归模型分析后,结果显示ePVS升高,心血管死亡(HR:1.085,95%CI:1.004~1.172,P=0.039)和主要不良心血管事件(HR:1.0516,95%CI:1.013~1.092,P=0.009)发生率增加。结论随着ePVS升高,心衰患者心血管死亡和主要不良心血管事件发生率均明显增加,ePVS是心衰患者发生心血管死亡和主要心血管不良事件的独立预测因子。Abstract: ObjectiveThe study was performed to evaluate the effect of estimated plasma volume status(ePVS) on the prognosis of patients with heart failure(HF).MethodsA total of 1448 patients with HF hospitalized in the Department of Cardiology, Affiliated Drum Tower Hospital, Medical School of Nanjing University from September 2010 to May 2019 were selected. We calculated ePVS at admission using the Duarte formula, derived from hemoglobin and hematocrit ratios. The patients were divided into two groups according to the median of ePVS. The association between ePVS and 1-year and 5-year cardiovascular mortality and incidence of major adverse cardiovascular events(MACE) were assessed.ResultsThere were statistically significant differences in 1-year and 5-year cardiovascular mortality between the low ePVS group and the high ePVS group(3.4% vs 8.3%, P < 0.001; 8.4% vs 16.5%, P < 0.001), the incidence of 1-year and 5-year major adverse cardiovascular events in the high ePVS group were higher than those in the low ePVS group(37.1% vs 29.8%, P=0.004; 66.4% vs 54.8%, P < 0.001). On multivariable Cox analysis, after adjusting for potential confounders, higher ePVS remained significantly associated with increased rate of cardiovascular death(HR: 1.085, 95%CI: 1.004-1.172, P=0.039) and incidence of MACE(HR: 1.0516, 95%CI: 1.013-1.092, P=0.009).ConclusionWith the increase of ePVS, the incidence of cardiovascular death and MACE in patients with HF increased significantly. The current study strengthened the evidence that ePVS had important prognostic value in patients with HF.
-
Key words:
- estimated plasma volume status /
- hemoglobin /
- hematocrit /
- heart failure /
- prognosis
-

-
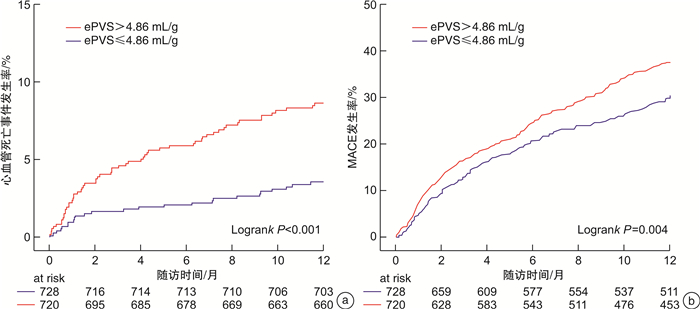
图 2 随访1年时不同ePVS分组心血管死亡和MACE发生率
Figure 2. Kaplan-Meier curves in incidence of cardiovascular death and MACE in one year
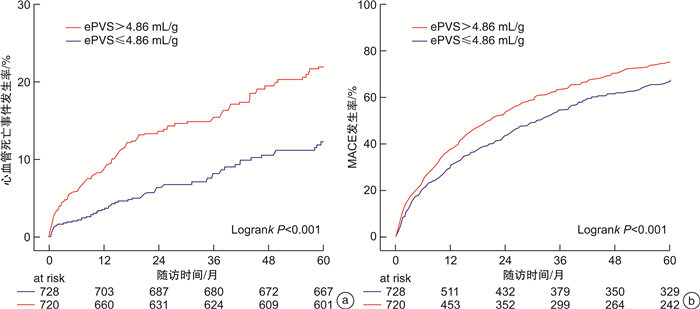
图 3 随访5年时不同ePVS分组心血管死亡和MACE发生率
Figure 3. Kaplan-Meier curves in incidence of cardiovascular death and MACE in five year
表 1 两组患者基线资料比较
Table 1. Baseline clinical characteristics
例(%), M(P25, P75) 项目 总体(1448例) ePVS分组 P值 ePVS低值组(728例) ePVS高值组(720例) 年龄/岁 74(64,81) 71(60,78) 77(68,83) < 0.001 女性 619(42.75) 222(30.51) 397(55.14) < 0.001 BMI/(kg·m-2) 24.00(22.00,25.00) 24.24(22.71,26.26) 23.87(21.74,24.44) < 0.001 住院天数/d 11(8,15) 10(7,14) 12(8,17) < 0.001 吸烟史 328(22.65) 202(27.75) 126(17.50) < 0.001 饮酒史 155(10.70) 109(14.97) 46(6.39) < 0.001 冠心病 546(37.71) 260(35.71) 286(39.72) 0.116 心瓣膜病 235(16.20) 106(14.60) 129(17.90) 0.083 心肌病 385(26.59) 202(23.75) 183(25.42) 0.316 心肌梗死史 202(13.95) 86(11.81) 116(16.11) 0.018 PCI/CABG史 263(18.16) 117(16.07) 146(20.28) 0.038 起搏器植入史 226(15.61) 104(14.29) 122(16.94) 0.163 高血压 970(66.99) 479(65.80) 491(68.19) 0.332 糖尿病 456(31.49) 185(25.41) 271(37.63) < 0.001 心房颤动 719(49.65) 361(49.59) 358(49.72) 0.959 卒中或TIA史 341(23.55) 154(21.15) 187(25.97) 0.031 肾功能不全 261(18.02) 68(9.34) 193(26.81) < 0.001 NYHA(Ⅲ/Ⅳ) 1142(78.87) 570(78.30) 572(79.44) 0.593 收缩压/mmHg△ 131(116,148) 130(117,147) 132(116,149) 0.571 舒张压/mmHg 76(66,86) 79(69,88) 72(64,82) < 0.001 心率/(次·min-1) 78(68,91) 78(68,92) 78(67,90) 0.050 肌酐/(μmol·L-1) 83(67,109) 81(66,98) 89(68,127) < 0.001 血钾/(mmol·L-1) 4.00(3.70,4.30) 3.92(3.64,4.21) 3.99(3.73,4.35) < 0.001 血钠/(mmol·L-1) 141.0(138.0,143.0) 141.0(138.3,142.9) 141.0(137.8,143.1) 0.715 总胆固醇/(mmol·L-1) 3.60(3.00,4.40) 3.82(3.18,4.49) 3.43(2.83,4.16) < 0.001 甘油三酯/(mmol·L-1) 1.00(0.80,1.50) 1.12(0.81,1.57) 1.00(0.72,1.36) < 0.001 LDL/(mmol·L-1) 1.9(1.5,2.5) 2.07(1.63,2.65) 1.73(1.31,2.28) < 0.001 HDL/(mmol·L-1) 1.0(0.8,1.2) 0.98(0.79,1.2) 0.94(0.76,1.18) 0.077 尿酸/(μmol·L-1) 428(337,539) 433(350,546) 420(323,535) 0.026 BNP/(pg·mL-1) 449(189,922) 416(169,847) 504(213,1055) < 0.001 HB/(g·L-1) 128(112,139) 139(133,149) 112(98,121) < 0.001 HCT/% 38.0(34.0,41.0) 40.8(38.8,42.7) 34.6(31.0,36.8) < 0.001 ePVS/(mL·g-1) 4.90(4.30,5.80) 4.25(3.89,4.56) 5.79(5.24,7.01) < 0.001 LVDd/cm 5.60(5.10,6.30) 5.75(5.13,6.50) 5.50(5.00,6.05) < 0.001 LVDs/cm 4.40(3.60,4.90) 4.39(3.75,5.14) 4.15(3.56,4.60) < 0.001 LAD/cm 4.80(4.40,5.30) 4.80(4.39,5.30) 4.80(4.34,5.30) 0.986 肺动脉压/mmHg 42(35,50) 40(35,50) 43(35,51) 0.001 LVEF/% 45(36,54) 43(33,53) 48(40,55) < 0.001 β受体阻滞剂 952(65.75) 508(69.78) 444(61.67) 0.001 CCB 301(20.79) 121(16.62) 180(25.00) < 0.001 ACEI/ARB 636(43.92) 338(46.43) 298(41.39) 0.053 利尿剂 1123(77.56) 560(76.92) 563(78.19) 0.562 醛固酮受体拮抗剂 841(58.08) 460(63.19) 381(52.92) < 0.001 洋地黄 282(19.48) 154(21.15) 128(17.78) 0.105 抗血小板药 693(47.86) 317(43.54) 376(52.22) 0.001 抗凝药 410(28.31) 235(32.28) 175(24.31) 0.001 他汀类 757(52.28) 377(51.79) 380(52.78) 0.706 注:BMI:体质指数;TIA:短暂性脑缺血发作;LDL:低密度脂蛋白;HDL:高密度脂蛋白;LVDd:左室舒张末期内径;LVDs:左室收缩末期内径;LAD:左房内径;△1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 终点事件发生情况
Table 2. End event occurrence
例(%) 终点事件 1年 5年 ePVS低值组 ePVS高值组 P值 ePVS低值组 ePVS高值组 P值 MACE 217(29.8) 267(37.1) 0.004 399(54.8) 478(66.4) < 0.001 心血管死亡 25(3.4) 60(8.3) < 0.001 61(8.4) 119(16.5) < 0.001 心肌梗死 8(1.1) 11(1.5) 0.473 19(2.6) 23(3.2) 0.508 心绞痛 17(2.3) 19(2.6) 0.711 35(4.8) 47(6.5) 0.157 心功能恶化 147(20.2) 151(21.0) 0.714 217(29.8) 235(32.6) 0.245 非致死性脑卒中 20(2.7) 26(3.6) 0.349 67(9.2) 54(7.5) 0.242
下载: 导出CSV
表 3 心血管死亡的Cox回归模型
Table 3. Cox regression analysis of cardiovascular death
因素 单因素 多因素 HR 95%CI P值 HR 95%CI P值 ePVS(每增加1mL/g) 1.151 1.089~1.216 < 0.001 1.085 1.004~1.172 0.039 性别(女性) 0.961 0.716~1.290 0.792 — — — 吸烟史 0.912 0.633~1.315 0.662 — — — 饮酒史 0.693 0.386~1.246 0.220 — — — 年龄(每增加1岁) 1.036 1.021~1.051 < 0.001 1.032 1.016~1.048 < 0.001 BMI(每增加1 kg/m2) 0.928 0.887~0.970 0.001 — — — 舒张压(每增加1 mmHg) 0.980 0.970~0.990 < 0.001 — — — 收缩压(每增加1 mmHg) 0.993 0.987~0.999 0.034 — — — 心率(每增加10次/min) 1.007 1.000~1.014 0.063 1.009 1.001~1.017 0.022 LVEF(每增加1%) 0.983 0.970~0.997 0.020 — — — 肺动脉压(每增加1 mmHg) 1.020 1.011~1.030 < 0.001 — — — 血肌酐(每增加1 μmol/L) 1.002 1.001~1.002 < 0.001 — — — 尿酸(每增加1 μmol/L) 1.002 1.002~1.003 < 0.001 1.002 1.001~1.002 0.001 BNP(每增加100 pg/mL) 1.049 1.038~1.061 < 0.001 1.036 1.021~1.052 < 0.001 NYHA(Ⅲ/Ⅳ) 2.257 1.477~3.450 < 0.001 — — — 冠心病 1.220 0.905~1.644 0.193 — — — 心肌梗死病史 2.291 1.630~3.220 < 0.001 2.037 1.388~2.991 0.000 高血压 1.047 0.764~1.435 0.776 — — — 糖尿病 1.465 1.086~1.977 0.013 1.422 1.031~1.962 0.032 心房颤动 1.096 0.817~1.470 0.542 — — — β受体阻滞剂 0.565 0.422~0.757 < 0.001 0.529 0.384~0.729 < 0.001 CCB 0.854 0.593~1.231 0.399 — — — ACEI/ARB 0.537 0.395~0.731 < 0.001 0.664 0.479~0.921 0.014 利尿剂 1.424 0.980~2.069 0.064 — — — 醛固酮受体拮抗剂 1.110 0.825~1.492 0.491 — — —
下载: 导出CSV
表 4 MACE的Cox回归模型
Table 4. Cox regression analysis of MACE
因素 单因素 多因素 HR 95%CI P值 HR 95% CI P值 ePVS(每增加1ml/g) 1.084 1.051~1.118 < 0.001 1.052 1.013~1.092 0.009 性别(女性) 1.027 0.899~1.173 0.700 — — — 吸烟史 0.900 0.764~1.060 0.208 — — — 饮酒史 0.910 0.723~1.147 0.426 — — — 年龄(每增加1岁) 1.018 1.013~1.024 < 0.001 1.019 1.012~1.026 < 0.001 BMI(每增加1kg/m2) 0.996 0.977~1.014 0.648 — — — 舒张压(每增加1mmHg) 0.994 0.989~0.999 0.014 — — — 收缩压(每增加1mmHg) 0.999 0.997~1.002 0.671 — — — 心率(每增加1次/分) 1.003 0.999~1.006 0.100 — — — LVEF(每增加1%) 0.984 0.978~0.990 < 0.001 0.985 0.977~0.993 < 0.001 肺动脉压(每增加1mmHg) 1.015 1.010~1.020 < 0.001 1.010 1.004~1.015 0.001 血肌酐(每增加1 μmol/L) 1.001 1.001~1.001 < 0.001 — — — 尿酸(每增加1 μmol/L) 1.001 1.001~1.002 < 0.001 1.001 1.000~1.001 0.011 BNP(每增加100 pg/ml) 1.027 1.020~1.034 < 0.001 1.012 1.004~1.020 0.005 NYHA(Ⅲ/Ⅳ) 1.787 1.503~2.124 < 0.001 1.333 1.108~1.605 0.002 冠心病 1.213 1.059~1.390 0.005 — — — 心梗病史 1.543 1.289~1.848 < 0.001 1.314 1.058~1.630 0.013 高血压 1.082 0.938~1.249 0.281 — — — 糖尿病 1.326 1.154~1.524 < 0.001 1.214 1.049~1.405 0.009 房颤 1.262 1.105-1.441 < 0.001 — — — β受体阻滞剂 0.968 0.844~1.111 0.647 — — — CCB 0.972 0.828~1.141 0.728 — — — ACEI/ARB 0.762 0.666~0.872 < 0.001 0.831 0.723~0.956 0.009 利尿剂 1.350 1.146~1.590 < 0.001 — — — 醛固酮受体拮抗剂 1.113 0.973~1.273 0.118 — — —
下载: 导出CSV
表 5 ePVS与结局事件的Cox回归模型
Table 5. Cox regression analysis of ePVS for outcome
因素 心血管死亡 MACE HR 95%CI P值 HR 95%CI P值 ePVS(连续性变量) 1.151 1.089~1.216 < 0.001 1.084 1.051~1.118 < 0.001 ePVS(≥4.86 mL/g vs < 4.86 mL/g) 2.051 1.506~2.792 < 0.001 1.284 1.124~1.467 < 0.001 ePVS(≥4.79 mL/g vs < 4.79 mL/g) 2.292 1.657~3.170 < 0.001 1.308 1.143~1.496 < 0.001 ePVS(≥4.61 mL/g vs < 4.61 mL/g) 2.102 1.496~2.953 < 0.001 1.374 1.195~1.580 < 0.001
下载: 导出CSV
-
[1] 廖玉华, 杨杰孚, 张健, 等. 舒张性心力衰竭诊断和治疗专家共识[J]. 临床心血管病杂志, 2020, 36(1): 1-10. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202001001.htm
[2] Gerber Y, Weston SA, Redfield MM, et al. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010[J]. JAMA Intern Med, 2015, 175(6): 996-1004. doi: 10.1001/jamainternmed.2015.0924
[3] Wang H, Chai K, Du M, et al. Prevalence and incidence of heart failure among urban patients in China: A national population-based analysis[J]. Circ Heart Fail. 2021, 14(10): e008406. doi: 10.1161/CIRCHEARTFAILURE.121.008406
[4] McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure[J]. N Engl J Med, 2014, 371(11): 993-1004. doi: 10.1056/NEJMoa1409077
[5] 中国心衰中心联盟. 舒张性心力衰竭早期防治专家建议[J]. 临床心血管病杂志, 2021, 37(1): 1-6. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202101001.htm
[6] McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction[J]. N Engl J Med, 2019, 381(21): 1995-2008. doi: 10.1056/NEJMoa1911303
[7] 王喆, 魏芳, 陈海燕, 等. 达格列净治疗心力衰竭疗效和安全性的Meta分析[J]. 临床心血管病杂志, 2021, 37(9): 854-861. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202109015.htm
[8] Ahlgrim C, Birkner P, Seiler F, et al. Estimated plasma volume status is a modest predictor of true plasma volume excess in compensated chronic heart failure patients[J]. Sci Rep, 2021, 11(1): 24235. doi: 10.1038/s41598-021-03769-9
[9] Kobayashi M, Girerd N, Duarte K, et al. Prognostic impact of plasma volume estimated from hemoglobin and hematocrit in heart failure with preserved ejection fraction[J]. Clin Res Cardiol, 2020, 109(11): 1392-1401. doi: 10.1007/s00392-020-01639-4
[10] Ling HZ, Flint J, Damgaard M, et al. Calculated plasma volume status and prognosis in chronic heart failure[J]. Eur J Heart Fail, 2015, 17(1): 35-43. doi: 10.1002/ejhf.193
[11] 中华医学会心血管病学分会心力衰竭学组, 中国医师协会心力衰竭专业委员会, 中华心血管病杂志编辑委员会. 中国心力衰竭诊断和治疗指南2018[J]. 中华心血管病杂志, 2018, 46(10): 760-789. doi: 10.3760/cma.j.issn.0253-3758.2018.10.004
[12] Bozkurt B, Coats AJS, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association[J]. Eur J Heart Fail, 2021, 23(3): 352-380. doi: 10.1002/ejhf.2115
[13] Duarte K, Monnez JM, Albuisson E, et al. Prognostic value of estimated plasma volume in heart failure[J]. JACC Heart Fail, 2015, 3(11): 886-893. doi: 10.1016/j.jchf.2015.06.014
[14] Rea ME, Dunlap ME. Renal hemodynamics in heart failure: implications for treatment[J]. Curr Opin Nephrol Hypertens, 2008, 17(1): 87-92.
[15] Ronco C, Haapio M, House AA, et al. Cardio renal syndrome[J]. J Am Coll Cardiol, 2008, 52(19): 1527-1539.
[16] Cadnapaphornchai MA, Gurevich AK, Weinberger HD, et al. Pathophysiology of sodium and water retention in heart failure[J]. Cardiology, 2001, 96(3-4): 122-131.
[17] Schrier RW, Abraham WT. Hormones and hemodynamics in heart failure[J]. N Engl J Med, 1999, 341(8): 577-585.
[18] 中国医师协会心力衰竭专业委员会, 中华心力衰竭和心肌病杂志编辑委员会. 心力衰竭容量管理中国专家建议[J]. 中华心力衰竭和心肌病杂志, 2018, 2(1): 8-16.
[19] Sherwi N, Pellicori P, Joseph AC, et al. Old and newer biomarkers in heart failure: from pathophysiology to clinical significance[J]. J Cardiovasc Med(Hagerstown), 2013, 14(10): 690-697.
[20] Lin Y, Xue Y, Liu J, et al. Prognostic value of estimated plasma volume in patients with chronic systolic heart failure[J]. J Investig Med, 2021, 69(2): 338-344.
[21] Rossignol P, Ménard J, Fay R, et al. Eplerenone survival benefits in heart failure patients post-myocardial infarction are independent from its diuretic and potassium-sparing effects. Insights from an EPHESUS(Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study)substudy[J]. J Am Coll Cardiol, 2011, 58(19): 1958-1966.
-
图(4)
表(5)
计量
- 文章访问数: 3056
- PDF下载数: 1064
- 施引文献: 0