
Development and validation of risk factors and its nomogram prediction model for short-term prognosis of fulminant myocarditis: a retrospective analysis
-
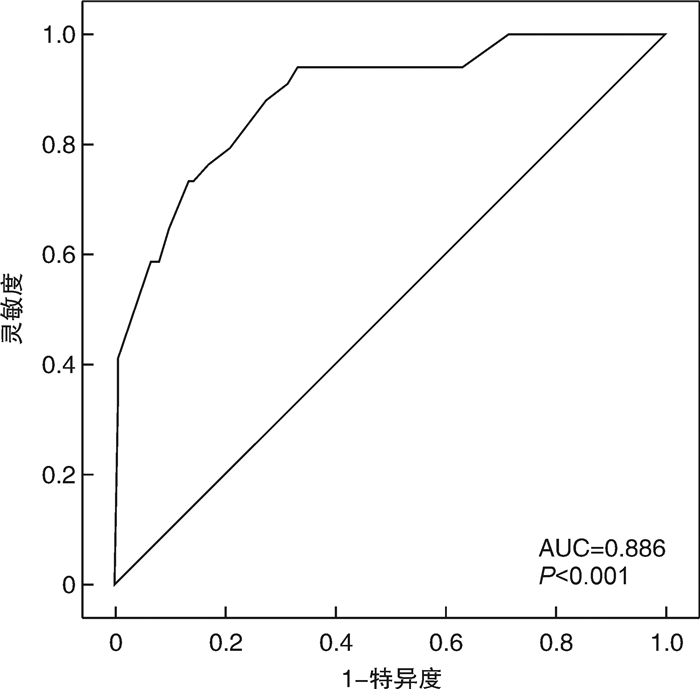
摘要: 目的 探讨影响暴发性心肌炎(FM)患者短期死亡的危险因素,构建列线图模型。方法 回顾性收集2015年10月—2020年11月住院治疗的157例FM患者的临床资料,将患者分为死亡组(34例)和存活组(123例),分析两组患者在年龄、性别、发病时长、并发恶性心律失常、既往病史、白细胞、总胆红素、估测肾小球滤过率(eGFR)、血清肌钙蛋白I(cTnI)峰值、B型钠尿肽前体、左室射血分数(LVEF)等指标方面是否存在差异。采用多因素logistic回归分析探讨影响FM近期死亡风险的独立危险因素,采用R4.1.1软件构建相关列线图模型,并采用校正曲线、C-index、ROC曲线等手段对该列线图模型进行验证。结果 多因素logistic回归分析显示,患者并发恶性心律失常(OR=5.352,95%CI 1.725~16.598)、eGFR < 85.77 mL·min-1·(1.73 m2)-1(OR=4.375,95%CI 1.167~16.394)、cTnI峰值≥26.75 μg/L(OR=4.258,95%CI 1.273~14.245)和LVEF < 40%(OR=4.790,95%CI 1.374~16.701)是预测FM患者近期死亡的独立危险因素。以上述各项指标建立的预测模型,经bootstrap法进行内部验证,其校正曲线趋近于理想曲线(P=0.110),表明该模型的一致性较好,该模型的C-index为0.886(95%CI 0.826~0.931),经过bootstrap法随机抽样验证后C-index调整为0.869,说明建立的模型拥有良好的区分度。模型的ROC曲线下面积为0.886,提示该模型有着良好的预测效能。结论 并发恶性心律失常、eGFR < 85.77 mL·min-1·(1.73 m2)-1、cTnI峰值≥26.75 μg/L以及LVEF < 40%的FM患者发病1个月内全因死亡的风险显著升高,由4项独立危险因素构建的列线图模型,有助于评估FM患者的近期预后。Abstract: Objective To explore the risk factors that affect the short-term death of fulminant myocarditis, and establish a nomogram model.Methods The clinical data of 157 patients with fulminant myocarditis who were hospitalized from October 2015 to November 2020 were retrospectively collected. They were divided into deaths group(34 cases) and survival group(123 cases). Then we analyzed whether there were differences of the age, gender, duration of onset, complicated with malignant arrhythmia, previous medical history, white blood cell, total bilirubin, estimated glomerular filtration rate(eGFR), the peak of chronic troponin I(cTnI), N-terminal Pro-B-type natriuretic peptide, left ventricular ejection fraction(LVEF) and other indicators between two groups. Multivariate logistic regression analysis was used to explore the independent risk factors affecting the recent mortality risk of fulminant myocarditis. The R language software(R 4.1. 1) was used to construct a nomogram model. The calibration curve, C-index and ROC curve were used to verify the nomogram model.Results Multivariate logistic regression analysis showed that complicated with malignant arrhythmia(OR=5.352, 95%CI: 1.725-16.598), eGFR < 85.77 mL·min-1·(1.73 m2)-1(OR=4.375, 95%CI: 1.167-16.394), the peak of cTnI≥26.75 μg/L(OR=4.258, 95%CI: 1.273-14.245) and LVEF < 40%(OR=4.790, 95%CI: 1.374-16.701) were independent risk factors for recent death of patients with fulminant myocarditis. The nomogram model established by the indicators above was verified by the bootstrap internal verification and its calibration curve is close to the ideal curve(P=0.110), indicating that the model was in good consistency. The C-index of the model was 0.886(95%CI: 0.826-0.931), and was adjusted to 0.869 after bootstrap verification, indicating good differentiation. The area under the ROC curve of the model was 0.886, indicating that the model had high efficacy of prediction.Conclusion The risk of all-caused death in patients with fulminant myocarditis combined with complicated with malignant arrhythmia, eGFR < 85.77 mL·min-1·(1.73 m2)-1, the peak of cTnI≥26.75 μg/L and LVEF < 40% was significantly increased within one month of onset. The nomogram established by four independent risk factors was helpful to assess the short-term prognosis of patients with fulminant myocarditis.
-
Key words:
- fulminant myocarditis /
- prognosis /
- risk factors /
- nomogram
-

-

图 1 预测FM患者1个月内全因死亡风险的列线图模型
Figure 1. The nomogram model for predicting short-term risk of all-cause mortality of FM
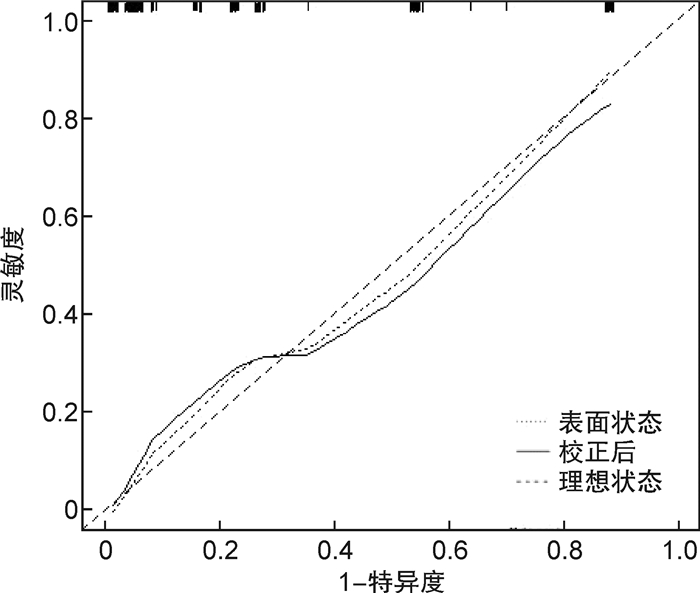
图 2 列线图模型预测FM预后的校正曲线
Figure 2. Calibration curve of nomogram model for predicting prognosis of FM
表 1 两组一般临床资料比较
Table 1. Basic data between two groups
X±S, M(P25, P75) 项目 死亡组(34例) 存活组(123例) P 男性/例(%) 22(64.7) 72(58.5) 0.516 年龄/岁 52±18 40±17 0.001 发病时长/d 2.0(1.0,4.3) 3.0(1.0,4.0) 0.529 住院时长/d 4.0(1.8,12.3) 13.0(9.0,18.0) < 0.001 前驱感染史/例(%) 29(85.3) 87(70.7) 0.087 并发恶性心律失常/例(%) 18(52.9) 18(14.6) < 0.001 既往史/例(%) 高血压 9(26.5) 22(17.9) 0.266 糖尿病 1(2.9) 13(10.6) 0.167 吸烟 7(20.6) 28(22.8) 0.787 酗酒 4(11.8) 16(13.0) 0.847 实验室检查 WBC/(×109·L-1) 11.55(7.18,15.91) 8.97(6.37,12.70) 0.159 Hb/(g·L-1) 131(118,154) 132(121,144) 0.693 eGFR/[mL·min-1·(1.73m2)-1] 57.91±33.44 99.04±39.86 < 0.001 UA/(μmol·L-1) 405.00(366.22,568.75) 338.00(255.60,433.10) 0.001 TBIL/(μmol·L-1) 18.73(12.43,29.12) 14.40(10.40,20.70) 0.014 cTnI峰值/(μg·L-1) 60.30(34.40,220.15) 25.90(6.54,131.70) 0.004 CRP/(mg·L-1) 14.54(13.23,15.39) 14.53(11.92,15.36) 0.166 NT-proBNP/(pg·mL-1) 11317(7136,32718) 6181(1944,10974) < 0.001 心电图/例(%) 病理性Q波 9(26.5) 34(27.6) 0.892 心电图ST-T动态改变 25(73.5) 75(61.0) 0.178 高度房室传导阻滞 5(14.7) 31(25.2) 0.197 心脏超声 LAD/mm 40(32,42) 36(32,39) 0.099 LVDd/mm 49(46,53) 49(46,53) 0.949 LVSd/mm 40(36,45) 37(32,41) 0.025 LVEF/% 34(31,39) 46(37,57) < 0.001 药物治疗/例(%) 糖皮质激素 29(85.3) 94(76.4) 0.266 丙种球蛋白 23(67.6) 83(67.5) 0.985 ACEI/ARB 9(26.5) 65(52.8) 0.004 利尿剂 20(58.8) 65(52.8) 0.536 多巴胺/多巴酚丁胺 24(70.6) 77(62.6) 0.390 去甲肾上腺素 26(76.5) 65(52.8) 0.014 机械循环支持/例(%) 临时起搏器 7(20.6) 26(21.1) 0.944 IABP 14(41.2) 27(22.0) 0.024 CRRT 11(32.4) 7(5.7) < 0.001 ECMO 4(11.8) 1(0.8) 0.001 IABP:主动脉球囊反搏。  下载: 导出CSV
下载: 导出CSV
表 2 变量转换赋值说明
Table 2. Description of variable conversion
自变量 赋值说明(所有连续性变量均计算约登指数确定截断值) 年龄 ≥37岁=1, < 37岁=0 并发恶性心律失常 并发恶性心律失常=1,未并发恶性心律失常=0 eGFR < 85.77 mL·min-1·(1.73m2)-1=1,≥85.77 mL·min-1·(1.73m2)-1=0 UA ≥373.65 μmol/L=1, < 373.65μmol/L=0 cTnI峰值 ≥26.75 μg/L=1, < 26.75 μg//L=0 TBIL ≥18.63 μmol/L=1, < 18.63 μmol/L=0 NT-proBNP ≥5820 pg/mL=1, < 5820 pg/mL=0 LVSd ≥37.5 mm=1, < 37.5 mm=0 LVEF < 40%=1,≥40%=0
下载: 导出CSV
表 3 FM短期死亡危险因素的多因素logistic回归分析
Table 3. Logistic regression analysis of risk factors associated with short-term mortality of FM
变量 SE Wald值 OR值 95%CI P 年龄 0.665 1.371 2.178 0.592-8.011 0.242 并发恶性心律失常 0.578 8.436 5.352 1.725-16.598 0.004 eGFR 0.674 4.794 4.375 1.167-16.394 0.029 UA 0.569 1.308 1.917 0.628-5.851 0.253 cTnI峰值 0.616 5.529 4.258 1.273-14.245 0.019 TBIL 0.527 0.425 1.410 0.502-3.966 0.514 NT-proBNP 0.713 0.112 0.788 0.195-3.190 0.738 LVSd 0.617 0.292 0.717 0.241-2.400 0.589 LVEF 0.637 6.045 4.790 1.374-16.701 0.014
下载: 导出CSV
-
[1] Liu L, Yang X, Gu Y, et al. Predictive value of the age, creatinine, and ejection fraction(ACEF)score in patients with acute fulminant myocarditis[J]. Front Physiol, 2021, 12: 596548. doi: 10.3389/fphys.2021.596548
[2] Hang W, Chen C, Seubert JM, et al. Fulminant myocarditis: a comprehensive review from etiology to treatments and outcomes[J]. Signal Transduct Target Ther, 2020, 5: 287. doi: 10.1038/s41392-020-00360-y
[3] 汪道文, 惠汝太. 推行暴发性心肌炎处理的中国方案, 挽救更多生命[J]. 中华心血管病杂志, 2022, 50(2): 212-218. https://xuewen.cnki.net/CCND-SGRB20220411A030.html
[4] Ammirati E, Cipriani M, Lilliu M et al. Survival and left ventricular function changes in fulminant versus nonfulminant acute myocarditis[J]. Circulation, 2017, 136: 529-545. doi: 10.1161/CIRCULATIONAHA.117.026386
[5] 严凤娣, 吴晓燕, 殷静静, 等. 体外膜肺氧合治疗急性暴发性心肌炎合并心源性休克16例临床分析[J]. 临床急诊杂志, 2021, 22(9): 521-524. doi: 10.13201/j.issn.1009-5918.2021.08.002
[6] 熊盟, 唐中建, 舒艾娅, 等. 清醒VA-ECMO联合心脏临时起搏及无创机械通气治疗暴发性心肌炎1例[J]. 临床急诊杂志, 2022, 23(9): 596-602. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202208010.htm
[7] 中华医学会心血管病学分会精准医学学组, 中华心血管病杂志编辑委员会, 成人暴发性心肌炎工作组, 等. 成人暴发性心肌炎诊断与治疗中国专家共识[J]. 中华心血管病杂志, 2017, 45(9): 742-752. doi: 10.3760/cma.j.issn.0253-3758.2017.09.004
[8] Everett BM. Cardiac troponin as a novel tool for cardiovascular risk prediction in ambulatory populations[J]. Trends Cardiovasc Med, 2017, 27: 41-47. doi: 10.1016/j.tcm.2016.06.002
[9] 左超, 卢秀兰, 陈智, 等. 肌钙蛋白T对暴发性心肌炎患儿病情评估的效能研究[J]. 临床急诊杂志, 2022, 23(10): 670-673. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202209012.htm
[10] Kazanski V, Mitrokhin VM, Mladenov MI, et al. Cytokine effects on mechano-induced electrical activity in atrial myocardium[J]. Immunol Invest, 2017, 46: 22-37. doi: 10.1080/08820139.2016.1208220
[11] Remels AHV, Derks WJA, Cillero-Pastor B, et al. NF-kappaB-mediated metabolic remodelling in the inflamed heart in acute viral myocarditis[J]. Biochim Biophys Acta Mol Basis Dis, 2018, 1864: 2579-2589. doi: 10.1016/j.bbadis.2018.04.022
[12] 蒋建刚, 刘超, 崔广林, 等. 暴发性心肌炎患者的长期预后及心功能受损的危险因素分析[J]. 中华心血管病杂志, 2022, 50(3): 263-269.
[13] Wu J, Zhang H, Gao Y, et al. Nursing effect of ECMO combined with CRRT in the treatment of fulminant myocarditis: A protocol of randomized controlled trial[J]. Medicine(Baltimore), 2021, 100: e24085.
[14] Agricola E, Marini C, Stella S, et al. Effects of functional tricuspid regurgitation on renal function and long-term prognosis in patients with heart failure[J]. J Cardiovasc Med(Hagerstown), 2017, 18: 60-68. doi: 10.2459/JCM.0000000000000312
[15] Landler NE, Mogelvang R, Bro S, et al. Kidney function and the prognostic value of myocardial performance index[J]. Int J Cardiovasc Imaging, 2021, 37: 1637-1647. doi: 10.1007/s10554-020-02149-0
[16] Chong SZ, Fang CY, Fang HY, et al. Associations with the in-hospital survival following extracorporeal membrane oxygenation in adult acute fulminant myocarditis[J]. J Clin Med, 2018, 7: 120.
[17] Li S, Xu S, Li C, et al. A life support-based comprehensive treatment regimen dramatically lowers the in-hospital mortality of patients with fulminant myocarditis: a multiple center study[J]. Sci China Life Sci, 2019, 62: 369-380.
[18] Zhou N, Zhao Y, Jiang J, et al. Impact of mechanical circulatory support and immunomodulation therapy on outcome of patients with fulminant myocarditis: Chinese registry of fulminant myocarditis[J]. Signal Transduct Target Ther, 2021, 6: 350.
-
图(3)
表(3)
计量
- 文章访问数: 1189
- PDF下载数: 311
- 施引文献: 0