
-
摘要: 随着影像技术的进步和有效治疗手段的不断涌现,心脏淀粉样变近年来备受关注。在当前临床实践中,仍存在对心脏淀粉样变认识不足、诊断技术普及率低、漏诊率和延迟诊断率高等问题。提高早期识别率、规范诊断流程、选择合理治疗方法对改善心脏淀粉样变的预后有重要意义。同时,临床上尚存在未满足的需求,亟待我们去探索和解决。Abstract: With the advancement of imaging technology and the emergence of effective treatment methods, cardiac amyloidosis has received much attention in recent years. However, in current domestic clinical practice, there are still problems such as insufficient understanding, low prevalence of diagnostic techniques, high rates of missed and delayed diagnosis. Improving the early recognition rate, standardizing the diagnostic process, and selecting reasonable treatment methods are important for improving the prognosis of cardiac amyloidosis. At the same time, there are still unmet clinical needs that need to be explored and solved.
-
Key words:
- cardiac amyloidosis /
- light-chain amyloidosis /
- transthyretin amyloidosis /
- diagnosis /
- treatment
-

-
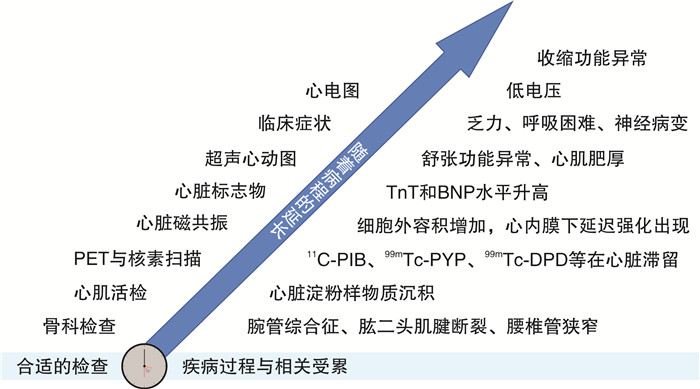
图 1 ATTR的疾病进程与相关检查
Figure 1. Proposed diagnostic tests based on typical disease process of ATTR
表 1 常见CA类型的表型特征
Table 1. Phenotypic characteristics in common types of CA
项目 AL ATTRm ATTRwt 心脏受累比例/% 70 30~100 100 平均诊断年龄/岁 60 60~70 76 男性比例/% 65 >80 >80 室间隔/左室后壁厚度/mm 15/14 17/16 18/17 LVEF/% 56 50 50 QRS低电压发生率/% 45 16~45 33 周围神经受累/% 10~20 15~54 < 10 自主神经受累/% 24 < 10 12~20 腕管综合征/% < 10 30~40 30~45 平均生存期/年 0.5(合并心力衰竭)~2.0 2~5 3.5~5.5  下载: 导出CSV
下载: 导出CSV
表 2 CA警示征
Table 2. Red flags and caveats in CA
类型 警示征 心脏相关 临床表现 高血压患者出现对降压药物不耐受或低血压;心肌肥厚家族史 心电图 出现不能解释的病理性Q波;与心肌肥厚不匹配的QRS波低电压;房室传导阻滞 实验室检查 NT-proBNP显著升高;持续cTnT水平升高 超声心动图 心肌颗粒样闪烁;合并右心室壁增厚或房间隔增厚或瓣膜增厚;心包积液;心尖保留的纵向应变率降低 心脏磁共振 心内膜下延迟强化;T1值升高;细胞外容积增加 心脏外 临床表现 合并神经病变:周围感觉/运动神经病变、自主神经功能障碍;合并骨科情况:腕管综合征、腰椎管狭窄、肱二头肌腱断裂、髋关节和膝关节置换术;多发性神经病变家族史 实验室检查 肾功能不全;蛋白尿 注:NT-proBNP:N末端脑钠肽前体;cTnT:心肌肌钙蛋白T。
下载: 导出CSV
表 3 不同CA预后分期
Table 3. Prognostic staging scores in AL and ATTR amyloidosis
项目 AL(梅奥)[19] ATTRwt(梅奥)[20] ATTRm和ATTRwt(英国)[21] 阳性预测指标 FLC差值≥18 mg/dL
TnT≥0.025 ng/mL
NT-proBNP≥1800 pg/mLTnT>0.05 ng/mL
NT-proBNP>3000 pg/mLeGFR < 45 mL/(min·1.73 m2)
NT-proBNP>3000 pg/mL分期与预后 分期标准 5年生存率 分期标准 中位生存时间 分期标准 中位生存时间 Ⅰ期(0项) 68% Ⅰ(0项) 66个月 Ⅰ(0项) 69.2个月 Ⅱ期(1项) 60% Ⅱ(1项) 40个月 Ⅱ(1项) 46.7个月 Ⅲ期(2项) 28% Ⅲ(2项) 20个月 Ⅲ(2项) 24.1个月 Ⅳ期(3项) 14% 注:eGFR:估测肾小球滤过率。
下载: 导出CSV
-
[1] Brownrigg JR, Leo V, Rose J, et al. Epidemiology of cardiomyopathies and incident heart failure in a population-based cohort study[J]. Heart, 2022, 108(17): 1383-1391. doi: 10.1136/heartjnl-2021-320181
[2] Merlo M, Pagura L, Porcari A, et al. Unmasking the prevalence of amyloid cardiomyopathy in the real world: results from Phase 2 of the AC-TIVE study, an Italian nationwide survey[J]. Eur J Heart Fail, 2022, 24(8): 1377-1386. doi: 10.1002/ejhf.2504
[3] 秦莹, 孙筱璐, 蒋文, 等. 心肌淀粉样变在心肌肥厚患者中的检出率及临床特点与预后分析[J]. 中国循环杂志, 2022, 37(6): 602-608. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202206005.htm
[4] Kyle RA, Linos A, Beard CM, et al. Incidence and natural history of primary systemic amyloidosis in Olmsted County, Minnesota, 1950 through 1989[J]. Blood, 1992, 79(7): 1817-1822. doi: 10.1182/blood.V79.7.1817.1817
[5] Hemminki K, Li X, Försti A, et al. Incidence and survival in non-hereditary amyloidosis in Sweden[J]. BMC Public Health, 2012, 12: 974. doi: 10.1186/1471-2458-12-974
[6] Tanskanen M, Peuralinna T, Polvikoski T, et al. Senile systemic amyloidosis affects 25% of the very aged and associates with genetic variation in alpha2-macroglobulin and tau: a population-based autopsy study[J]. Ann Med, 2008, 40(3): 232-239. doi: 10.1080/07853890701842988
[7] Castano A, Haq M, Narotsky DL, et al. Multicenter Study of Planar Technetium 99 m Pyrophosphate Cardiac Imaging: Predicting Survival for Patients With ATTR Cardiac Amyloidosis[J]. JAMA Cardiol, 2016, 1(8): 880-889. doi: 10.1001/jamacardio.2016.2839
[8] González-López E, Gallego-Delgado M, Guzzo-Merello G, et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction[J]. Eur Heart J, 2015, 36(38): 2585-2594. doi: 10.1093/eurheartj/ehv338
[9] Mohammed SF, Mirzoyev SA, Edwards WD, et al. Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction[J]. JACC Heart Fail, 2014, 2(2): 113-122. doi: 10.1016/j.jchf.2013.11.004
[10] Maurer MS, Elliott P, Comenzo R, et al. Addressing Common Questions Encountered in the Diagnosis and Management of Cardiac Amyloidosis[J]. Circulation, 2017, 135(14): 1357-1377. doi: 10.1161/CIRCULATIONAHA.116.024438
[11] Garcia-Pavia P, Rapezzi C, Adler Y, et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases[J]. Eur J Heart Fail, 2021, 23(4): 512-526. doi: 10.1002/ejhf.2140
[12] Cyrille NB, Goldsmith J, Alvarez J, et al. Prevalence and prognostic significance of low QRS voltage among the three main types of cardiac amyloidosis[J]. Am J Cardiol, 2014, 114(7): 1089-1093. doi: 10.1016/j.amjcard.2014.07.026
[13] Maurer MS, Bokhari S, Damy T, et al. Expert Consensus Recommendations for the Suspicion and Diagnosis of Transthyretin Cardiac Amyloidosis[J]. Circ Heart Fail, 2019, 12(9): e006075. doi: 10.1161/CIRCHEARTFAILURE.119.006075
[14] Kittleson MM, Maurer MS, Ambardekar AV, et al. Cardiac Amyloidosis: Evolving Diagnosis and Management: A Scientific Statement From the American Heart Association[J]. Circulation, 2020, 142(1): e7-e22. doi: 10.1161/CIRCULATIONAHA.120.047293
[15] Palladini G, Russo P, Bosoni T, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine[J]. Clin Chem, 2009, 55(3): 499-504. doi: 10.1373/clinchem.2008.117143
[16] Fine NM, Arruda-Olson AM, Dispenzieri A, et al. Yield of noncardiac biopsy for the diagnosis of transthyretin cardiac amyloidosis[J]. Am J Cardiol, 2014, 113(10): 1723-1727. doi: 10.1016/j.amjcard.2014.02.030
[17] Gillmore JD, Maurer MS, Falk RH, et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis[J]. Circulation, 2016, 133(24): 2404-2412. doi: 10.1161/CIRCULATIONAHA.116.021612
[18] Nativi-Nicolau J, Maurer MS. Amyloidosis cardiomyopathy: update in the diagnosis and treatment of the most common types[J]. Curr Opin Cardiol, 2018, 33(5): 571-579. doi: 10.1097/HCO.0000000000000547
[19] Kumar S, Dispenzieri A, Lacy MQ, et al. Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements[J]. J Clin Oncol, 2012, 30(9): 989-995. doi: 10.1200/JCO.2011.38.5724
[20] Grogan M, Scott CG, Kyle RA, et al. Natural History of Wild-Type Transthyretin Cardiac Amyloidosis and Risk Stratification Using a Novel Staging System[J]. J Am Coll Cardiol, 2016, 68(10): 1014-1020. doi: 10.1016/j.jacc.2016.06.033
[21] Gillmore JD, Damy T, Fontana M, et al. A new staging system for cardiac transthyretin amyloidosis[J]. Eur Heart J, 2018, 39(30): 2799-2806. doi: 10.1093/eurheartj/ehx589
[22] Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines[J]. Circulation, 2022, 145(18): e876-e894.
[23] Adams D, Gonzalez-Duarte A, O'Riordan WD, et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis[J]. N Engl J Med, 2018, 379(1): 11-21. doi: 10.1056/NEJMoa1716153
[24] Benson MD, Waddington-Cruz M, Berk JL, et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis[J]. N Engl J Med, 2018, 379(1): 22-31. doi: 10.1056/NEJMoa1716793
[25] El-Am EA, Dispenzieri A, Melduni RM, et al. Direct Current Cardioversion of Atrial Arrhythmias in Adults With Cardiac Amyloidosis[J]. J Am Coll Cardiol, 2019, 73(5): 589-597. doi: 10.1016/j.jacc.2018.10.079
-

图(2)
表(3)
计量
- 文章访问数: 1706
- PDF下载数: 667
- 施引文献: 0