
Effects of percutaneous coronary intervention and recovery of left ventricular ejection fraction on the prognosis of patients with chronic total occlusion and heart failure with a mildly reduced ejection fraction
-
摘要: 目的 探讨成功经皮冠状动脉介入治疗慢性完全闭塞病变(CTO-PCI)和左室射血分数(left ventricular ejection fraction,LVEF)恢复对CTO合并射血分数轻度降低的心力衰竭(heart failure with mildly reduced ejection fraction,HFmrEF)患者预后的影响,并探讨LVEF恢复的影响因素。方法 选取2018年1月—2019年3月于郑州大学第一附属医院就诊的CTO合并HFmrEF且接受PCI治疗的患者138例,根据CTO是否开通分为开通组(63例)和未开通组(75例)。将随访患者治疗1年后LVEF≥50%定义为LVEF恢复,收集并比较2组患者基线资料、治疗后3年内主要心脑血管不良事件(major adverse cardiac and cerebrovascular events,MACCE)发生情况,包括全因死亡、心源性死亡、非致死性心肌梗死、再次血运重建、心力衰竭再住院及脑卒中。结果 治疗3年后开通组总MACCE发生率低于未开通组(22.2% vs 46.7%,P=0.003)。Kaplan-Meier曲线显示开通组治疗后3年内总MACCE累积发生率低于未开通组(log-rank P=0.003)。多因素Cox回归分析显示CTO-PCI(HR=0.524,95%CI:0.277~0.991,P=0.047)和LVEF恢复(HR=0.498,95%CI:0.256~0.971,P=0.041)是治疗后3年内总MACCE发生的独立保护因素。多因素logistic回归显示CTO-PCI、eGFR和基线LVEF是治疗1年后LVEF恢复的独立影响因素(均P < 0.05)。结论 CTO-PCI开通CTO病变和LVEF恢复的CTO合并HFmrEF患者的MACCE发生率更低,预后更好。CTO-PCI、eGFR和基线LVEF是LVEF恢复的独立影响因素。
-
关键词:
- 经皮冠状动脉介入治疗 /
- 左室射血分数恢复 /
- 慢性完全闭塞病变 /
- 射血分数轻度降低的心力衰竭 /
- 预后
Abstract: Objective To explore the effect of the successful percutaneous coronary intervention for chronic total occlusion(CTO-PCI) and recovery of left ventricular ejection fraction(LVEF) on the prognosis of patients with CTO and heart failure with mildly reduced ejection fraction(HFmrEF), and to explore the influencing factors of LVEF recovery.Methods A total of 138 patients with CTO combined with HFmrEF who received PCI treatment in the First Affiliated Hospital of Zhengzhou University from January 2018 to March 2019 were selected and divided into the open group(n=63) and the unopened group(n=75) according to whether the CTO lesions were opened or not. LVEF≥50% after 1 year of follow-up treatment was defined as LVEF, and the baseline data and the incidence of major adverse cardiovascular and cerebrovascular events(MACCE) within 3 years after treatment were collected and compared between the two groups, including all-cause death, cardiac death, non-fatal myocardial infarction, revascularization, heart failure rehospitalization and stroke.Results After 3 years of treatment, the incidence of total MACCE in the open group was lower than that in the unopened group(P=0.003). The Kaplan-Meier curve showed that the cumulative incidence of total MACCE within 3 years after treatment in the open group was lower than that in the unopened group(log-rank P=0.003). Multivariate Cox regression analysis showed that CTO-PCI(HR=0.524, 95%CI: 0.277-0.991, P=0.047) and LVEF recovery(HR=0.498, 95%CI: 0.256-0.971, P=0.041) were independent protective factors for the development of total MACCE within 3 years after treatment. Multivariate logistic regression showed that CTO-PCI, eGFR and baseline LVEF were independent influencing factors of LVEF recovery after 1 year of treatment(all P < 0.05).Conclusion CTO-PCI opening CTO lesions and LVEF recovery are associated with lower MACCE incidence and better prognosis in patients with CTO and HFmrEF. CTO-PCI, eGFR, and baseline LVEF were independent factors for LVEF recovery. -

-
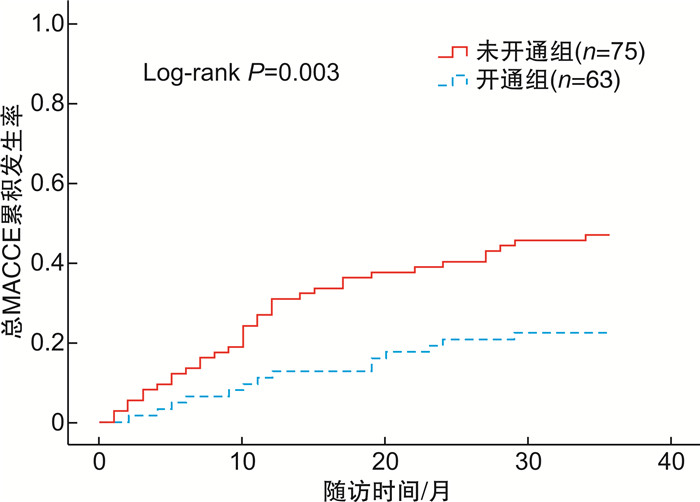
图 1 2组患者治疗后3年内总MACCE累积发生率Kaplan-Meier曲线
Figure 1. Kaplan-Meier curve of cumulative incidences of total MACCE within 3 years after treatment between two groups
表 1 2组患者基线资料比较
Table 1. Comparison of baseline data between two groups
例(%), X±S, M(P25, P75) 项目 开通组(63例) 未开通组(75例) t/χ2/Z P值 一般资料 年龄/岁 64.24±11.23 65.35±9.91 0.616 0.539 男性 44(69.8) 53(70.7) 0.011 0.916 体重指数/(kg·m-2) 23.94±1.63 23.73±0.75 0.965 0.336 高血压 35(55.6) 45(60.0) 0.278 0.598 冠心病家族史 8(12.7) 9(12.0) 0.015 0.901 糖尿病 16(25.4) 29(38.7) 2.744 0.098 吸烟史 25(39.7) 35(46.7) 0.680 0.410 卒中史 17(27.0) 11(14.7) 3.212 0.073 既往心肌梗死病史 23(36.5) 31(41.3) 0.335 0.563 外周动脉粥样硬化 21(33.3) 31(41.3) 0.933 0.334 心律失常 11(17.5) 22(29.3) 2.653 0.103 检验结果 血红蛋白/(g·L-1) 132.43±14.93 129.07±16.22 1.259 0.210 总胆固醇/(mmol·L-1) 3.72±0.83 3.59±0.83 0.885 0.378 甘油三酯/(mmol·L-1) 1.26(1.01,2.01) 1.16(0.95,1.53) 1.007 0.314 HDL-C/(mmol·L-1) 1.02±0.26 1.00±0.28 0.341 0.734 LDL-C/(mmol·L-1) 2.37±0.80 2.22±0.73 1.147 0.253 eGFR/[mL·min-1·(1.73m2)-1] 88.33±14.38 83.53±17.43 1.742 0.084 NT-proBNP/(ng·L-1) 1579.0(1214.0,2900.0) 1860.0(1231.9,2581.5) 0.562 0.574 基线LVEF/% 45.53±2.67 45.39±2.68 0.094 0.759 用药情况 螺内酯 34(54.0) 45(60.0) 0.509 0.476 β受体阻滞剂 54(85.7) 58(77.3) 1.573 0.210 ACEI/ARB/ARNI 41(65.1) 57(76.0) 1.984 0.159 利尿剂 28(44.4) 38(50.7) 0.509 0.476 介入手术资料 Rentrop分级≥2级 33(52.4) 35(46.7) 0.447 0.504 SYNTAX评分/分 23.18±5.97 22.96±5.97 0.210 0.834 J-CTO评分/分 1.35±0.65 1.37±0.60 0.163 0.871 CTO病变位置 前降支 34/79(43.0) 29/114(25.4) 6.574 0.010 回旋支 17/79(21.5) 39/114(34.2) 3.649 0.056 右冠脉 28/79(35.4) 46/114(40.4) 0.475 0.490 冠脉多支病变 52(82.5) 71(94.7) 5.197 0.023 手术并发症 13(20.6) 2/9(22.2) 0.000 1.000  下载: 导出CSV
下载: 导出CSV
表 2 LVEF恢复的多因素logistic回归分析
Table 2. Multivariate logistic regression analysis of LVEF recovery
变量 OR 95%CI P值 CTO-PCI 2.371 1.114~5.049 0.025 eGFR 1.032 1.004~1.061 0.027 基线LVEF 1.314 1.129~1.529 < 0.001
下载: 导出CSV
表 3 2组患者治疗3年后MACCE发生情况
Table 3. Incidences of MACCE between two groups after 3 years of treatment
例(%) 项目 开通组
(63例)未开通组
(75例)χ2 P值 全因死亡 3(4.8) 6(8.0) 0.178 0.674a) 心源性死亡 2(3.2) 4(5.3) 0.040 0.841a) 非致死性心肌梗死 5(7.9) 10(13.3) 1.029 0.310 再次血运重建 7(11.1) 17(22.7) 3.182 0.074 心衰再住院 6(9.5) 13(17.3) 1.759 0.185 脑卒中 2(3.2) 3(4.0) 0.000 1.000a) 总MACCE 14(22.2) 35(46.7) 8.934 0.003 注:a)采用校正χ2检验。
下载: 导出CSV
表 4 总MACCE的多因素Cox回归分析
Table 4. Multivariate Cox regression analysis of total MACCE
变量 HR 95%CI P值 CTO-PCI 0.524 0.277~0.991 0.047 LVEF恢复 0.498 0.256~0.971 0.041 糖尿病 2.043 1.137~3.670 0.017
下载: 导出CSV
-
[1] Bozkurt B, Coats A, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association[J]. Eur J Heart Fail, 2021, 23(3): 352-380. doi: 10.1002/ejhf.2115
[2] Shang Z, Wang X, Gao W. Heart failure with mildly reduced ejection fraction: emerging frontiers in clinical characteristics, prognosis, and treatment[J]. Rev Cardiovasc Med, 2022, 23(1): 30.
[3] 王华, 李莹莹, 柴坷, 等. 中国住院心力衰竭患者流行病学及治疗现状[J]. 中华心血管病杂志, 2019(11): 865-874.
[4] Koelbl CO, Nedeljkovic ZS, Jacobs AK. Coronary Chronic Total Occlusion(CTO): A Review[J]. Rev Cardiovasc Med, 2018, 19(1): 33-39. doi: 10.1016/j.carrev.2017.05.003
[5] Galassi AR, Brilakis ES, Boukhris M, et al. Appropriateness of percutaneous revascularization of coronary chronic total occlusions: an overview[J]. Eur Heart J, 2016, 37(35): 2692-2700. doi: 10.1093/eurheartj/ehv391
[6] 申学谦, 史雨晨, 见闻, 等. 冠状动脉慢性完全闭塞中胶原酶辅助介入治疗研究进展[J]. 临床心血管病杂志, 2022, 38(12): 951-954. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202212005.htm
[7] Werner GS, Martin-Yuste V, Hildick-Smith D, et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions[J]. Eur Heart J, 2018, 39(26): 2484-2493. doi: 10.1093/eurheartj/ehy220
[8] Brilakis ES, Mashayekhi K, Burke MN. How DECISION-CTO Can Help Guide the Decision to Perform Chronic Total Occlusion Percutaneous Coronary Intervention[J]. Circulation, 2019, 139(14): 1684-1687. doi: 10.1161/CIRCULATIONAHA.119.039835
[9] Obedinskiy AA, Kretov EI, Boukhris M, et al. The IMPACTOR-CTO Trial[J]. JACC Cardiovasc Interv, 2018, 11(13): 1309-1311. doi: 10.1016/j.jcin.2018.04.017
[10] Patel MR, Marso SP, Dai D, et al. Comparative effectiveness of drug-eluting versus bare-metal stents in elderly patients undergoing revascularization of chronic total coronary occlusions: results from the National Cardiovascular Data Registry, 2005-2008[J]. JACC Cardiovasc Interv, 2012, 5(10): 1054-1061. doi: 10.1016/j.jcin.2012.05.017
[11] Khan AA, Khalid MF, Ayub MT, et al. Outcomes of Percutaneous Coronary Intervention Versus Optimal Medical Treatment for Chronic Total Occlusion: A Comprehensive Meta-analysis[J]. Curr Probl Cardiol, 2021, 46(3): 100695. doi: 10.1016/j.cpcardiol.2020.100695
[12] 畅晓燕, 赵江峰. 经皮冠状动脉介入治疗慢性完全闭塞病变对患者心脏功能的影响[J]. 临床心血管病杂志, 2021, 37(3): 220-223. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202103007.htm
[13] Ybarra LF, Rinfret S. Why and How Should We Treat Chronic Total Occlusion? Evolution of State-of-the-Art Methodsand Future Directions[J]. Can J Cardiol, 2022, 38(10 Suppl1): S42-S53.
[14] 于子翔, 董佳佳, 赵龙, 等. 冠状动脉慢性完全闭塞病变侧支循环的预测因素和预后意义[J]. 临床心血管病杂志, 2021, 37(8): 705-709. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202108005.htm
[15] de Marchi SF, Streuli S, Haefeli P, et al. Determinants of prognostically relevant intracoronary electrocardiogram ST-segment shift during coronary balloon occlusion[J]. Am J Cardiol, 2012, 110(9): 1234-1239. doi: 10.1016/j.amjcard.2012.06.023
[16] Lee SW, Lee PH, Ahn JM, et al. Randomized Trial Evaluating Percutaneous Coronary Intervention for the Treatment of Chronic Total Occlusion[J]. Circulation, 2019, 139(14): 1674-1683. doi: 10.1161/CIRCULATIONAHA.118.031313
[17] Wybraniec MT, Orszulak M, Męcka K, et al. Heart Failure with Improved Ejection Fraction: Insight into the Variable Nature of Left Ventricular Systolic Function[J]. Int J Environ Res Public Health, 2022, 19(21): 14400. doi: 10.3390/ijerph192114400
[18] Perry A, Loh F, Adamo L, et al. Unsupervised cluster analysis of patients with recovered left ventricular ejection fraction identifies unique clinical phenotypes[J]. PLoS One, 2021, 16(3): e0248317.
[19] Kalogeropoulos AP, Fonarow GC, Georgiopoulou V, et al. Characteristics and Outcomes of Adult Outpatients With Heart Failure and Improved or Recovered Ejection Fraction[J]. JAMA Cardiol, 2016, 1(5): 510-518.
[20] Savarese G, Vedin O, D'Amario D, et al. Prevalence and Prognostic Implications of Longitudinal Ejection Fraction Change in Heart Failure[J]. JACC Heart Fail, 2019, 7(4): 306-317.
[21] Basuray A, French B, Ky B, et al. Heart failure with recovered ejection fraction: clinical description, biomarkers, and outcomes[J]. Circulation, 2014, 129(23): 2380-2387.
[22] Cardona M, Martín V, Prat-Gonzalez S, et al. Benefits of chronic total coronary occlusion percutaneous intervention in patients with heart failure and reduced ejection fraction: insights from a cardiovascular magnetic resonance study[J]. J Cardiovasc Magn Reson, 2016, 18(1): 78.
[23] Henriques JP, Hoebers LP, Råmunddal T, et al. Percutaneous Intervention for Concurrent Chronic Total Occlusions in Patients With STEMI: The EXPLORE Trial[J]. J Am Coll Cardiol, 2016, 68(15): 1622-1632.
-
图(1)
表(4)
计量
- 文章访问数: 2156
- PDF下载数: 1095
- 施引文献: 0