
-
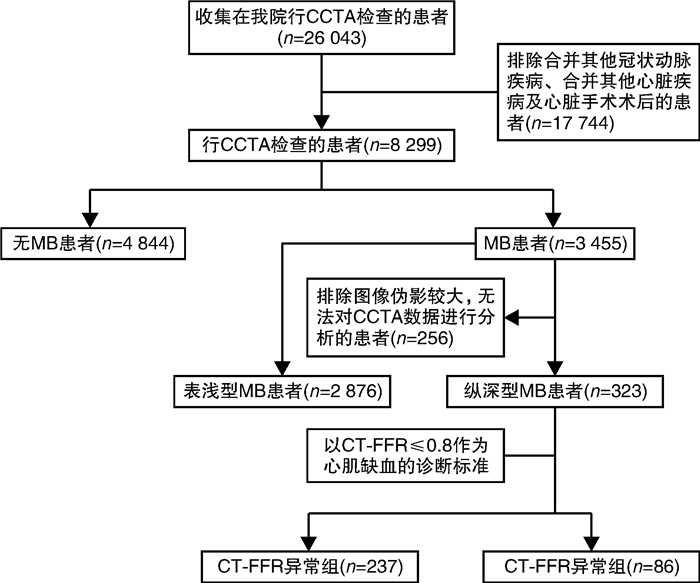
摘要: 目的 通过冠状动脉CT血管造影(coronary CT angiography,CCTA)检查探讨左冠状动脉前降支(left anterior descending coronary artery,LAD)纵深型心肌桥(myocardial bridging,MB)形态与CT血流储备分数(CT-FFR)的关系。方法 回顾性分析2018年1月—2022年4月包头医学院第一附属医院影像科323例LAD纵深型MB患者的解剖学信息,并以CT-FFR≤0.80为心肌缺血的指标,将患者分为CT-FFR正常组(237例)及CT-FFR异常组(86例)。采用t检验分析比较2组各MB参数的差异,采用岭回归模型分析CT-FFR值的影响因素,通过ROC曲线分析差异有统计学意义的参数。结果 2组MB入口处位置、出口处位置、长度、肌肉指数、收缩期压迫程度及壁冠状动脉(mural coronary artery,MCA)最狭窄处面积、入口处面积、出口处面积差异均有统计学意义(P < 0.05)。岭回归方程显示,MB出口位置、长度及肌肉指数对CT-FFR值具有负向影响(P < 0.05),MCA面积对CT-FFR值具有正向影响(P < 0.05),并且MB长度、出口位置、肌肉指数对MB心肌缺血均具有较高的诊断价值,三者的曲线下面积(AUC)分别为0.85、0.80、0.79。结论 LAD纵深型MB的位置离冠状窦越近、MCA面积越窄,尤其是MB长度较长的患者,更容易出现心肌缺血的临床表现,应予以高度重视。
-
关键词:
- 心肌桥 /
- 冠状动脉CT血管成像 /
- 心肌缺血 /
- 血流储备分数
Abstract: Objective To investigate the correlation between the Morphology of deep myocardial bridges (MB) over the left anterior descending coronary artery (LAD) and the measurement of coronary fractional flow reserve derived from CT (CT-FFR) by coronary CT angiography (CCTA).Methods The anatomical information of 323 patients with LAD deep MB in the First Affiliated Hospital of Baotou Medical College from January 2018 to April 2022 were retrospectively analyzed. With CT-FFR≤0.80 as the index for myocardial ischemia, the patients were divided into the normal CT-FFR group (n=237) and the abnormal CT-FFR group (n=86). MB parameters were analyzed and compared between the two groups using the t test. The influencing factors of CT-FFR values were analyzed by a multivariate linear regression model, and the parameters with statistically significant differences were analyzed with the ROC curve.Results Statistically significant differences were found between the two groups in the entrance location, exit location, length, muscle index and systolic compression degree of MB, as well as the areas of the narrowest part, entrance and exit of mural coronary artery (MCA) (P < 0.05). The ridge regression equation showed that the exit location, length and muscle index of MB had a negative effect on CT-FFR values (P < 0.05), while the area of the MCA had a positive effect on CT-FFR values (P < 0.05). Additionally, the length, exit location and muscle index of MB presented high diagnostic values for myocardial ischemia, with the area under the curve (AUC) of 0.85, 0.80 and 0.79, respectively.Conclusion The closer the position of LAD deep MB is to the coronary sinus, the narrower the MCA area is, and especially the MB patients with longer MB length are more likely to have clinical manifestations of myocardial ischemia, which should be paid more attention to. -

-
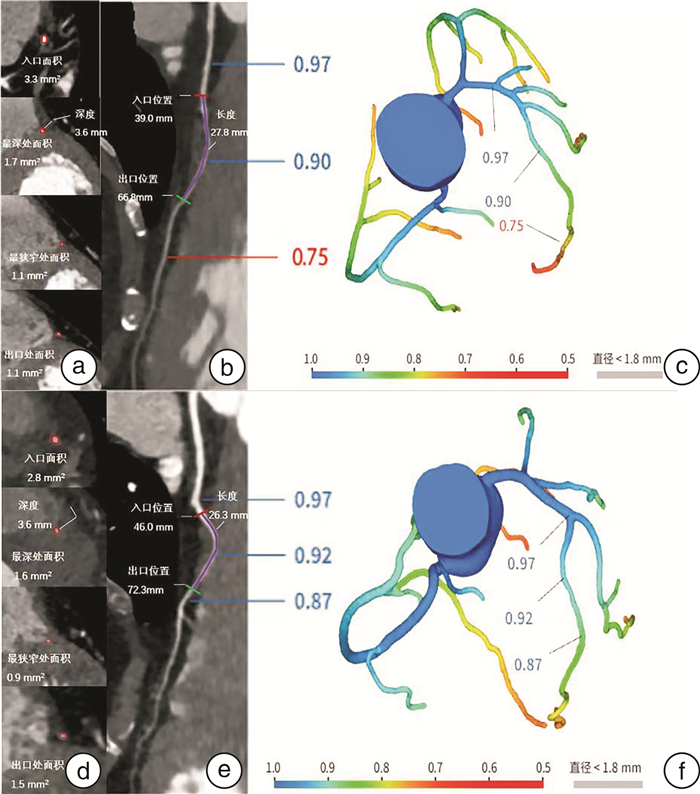
图 2 MB位置、长度、深度、MCA面积及CT-FFR值测量图
Figure 2. MB position, length, depth, MCA area and CT-FFR value measurement map
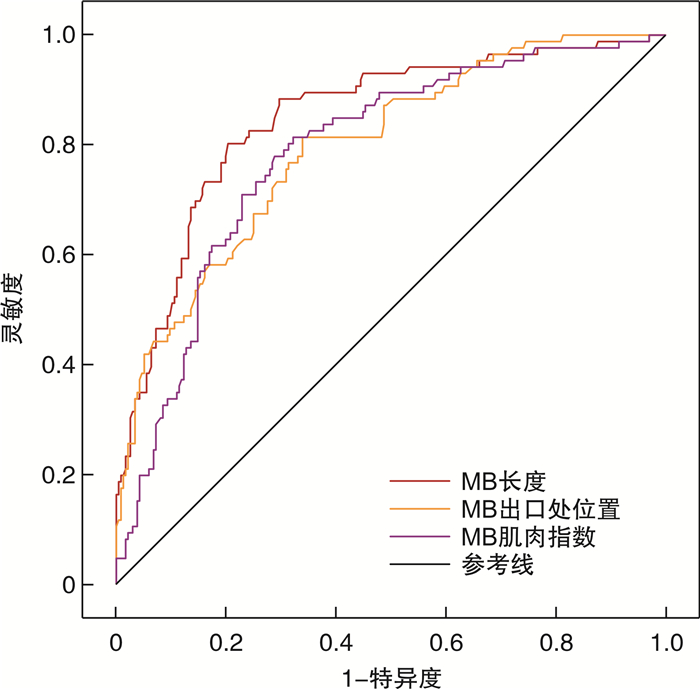
图 3 MB解剖学参数诊断CT-FFR异常效能的ROC曲线
Figure 3. ROC curve of MB anatomical parameters for diagnosing CT-FFR abnormalities
表 1 2组LAD纵深型MB患者CCTA解剖学参数比较
Table 1. Comparison of anatomical parameters of CCTA in two groups of patients with LAD deep MB
X±S 参数 CT-FFR正常组(237例) CT-FFR异常组(86例) t值 P值 MB入口位置/mm 47.8±10.1 44.8±8.9 -2.422 0.016 MB最深处位置/mm 58.9±11.0 58.2±12.0 -0.547 0.585 MB出口位置/mm 78.7±12.5 95.7±18.2 8.038 < 0.001 MB长度/mm 30.8±11.1 49.8±16.4 10.001 < 0.001 MB深度/mm 3.6±1.7 4.2±2.8 1.970 0.052 MB肌肉指数 115.4±79.8 231.8±317.6 3.361 0.001 MCA收缩期压迫指数/% 42.5±11.5 45.8±10.9 2.287 0.023 MCA最狭窄处面积/mm2 1.8±0.7 1.4±0.5 -5.270 < 0.001 MCA最深处面积/mm2 2.5±1.1 2.2±1.3 -1.995 0.047 MCA入口处面积/mm2 5.1±2.2 4.6±2.4 -1.555 0.121 MCA出口处面积/mm2 2.4±0.9 2.0±0.7 -4.722 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 影响MB患者CT-FFR值的岭回归分析
Table 2. Ridge Regression analysis affecting CT-FFR value in MB patients
参数 非标准化系数 标准化系数 t值 P值 B 标准误 β 常数 0.870 0.010 - 86.751 < 0.001 MB入口位置 0.000 0.000 0.028 1.753 0.081 MB最深处位置 0.000 0.000 0.001 0.034 0.973 MB出口处位置 -0.001 0.000 -0.187 -12.063 < 0.001 MB长度 -0.001 0.000 -0.199 -13.181 < 0.001 MB深度 0.000 0.000 0.009 0.557 0.578 MB肌肉指数 0.001 0.000 -0.081 -5.278 < 0.001 MCA最狭窄处面积 0.009 0.001 0.126 7.966 < 0.001 MCA最深处面积 0.003 0.001 0.067 3.740 < 0.001 MCA入口处面积 0.002 0.000 0.093 5.882 < 0.001 MCA出口处面积 0.006 0.001 0.100 5.473 < 0.001 MCA收缩期压迫指数 0.000 0.000 -0.005 -0.299 0.765 R2 0.503 调整R2 0.485 F F(11,310)=28.465,P < 0.001
下载: 导出CSV
-
[1] Tarantini G, Migliore F, Cademartiri F, et al. Left Anterior Descending Artery Myocardial Bridging: A Clinical Approach[J]. J Am Coll Cardiol, 2016, 68(25): 2887-2899. doi: 10.1016/j.jacc.2016.09.973
[2] 王兰, 周子华, 郭瑄, 等. 114例心肌桥患者焦虑抑郁状况及其相关危险因素分析[J]. 临床心血管病杂志, 2018, 34(2): 162-165. doi: 10.13201/j.issn.1001-1439.2018.02.014
[3] Zhao DH, Fan Q, Ning JX, et al. Myocardial bridge-related coronary heart disease: Independent influencing factors and their predicting value[J]. World J Clin Cases, 2019, 7(15): 1986-1995. doi: 10.12998/wjcc.v7.i15.1986
[4] Kim YJ, Yong HS, Kim SM, et al. Korean guidelines for the appropriate use of cardiac CT[J]. Korean J Radiol, 2015, 16(2): 251-285. doi: 10.3348/kjr.2015.16.2.251
[5] Fairbairn TA, Nieman K, Akasaka T, et al. Real-world clinical utility and impact on clinical decision-making of coronary computed tomography angiography-derived fractional flow reserve: lessons from the ADVANCE Registry[J]. Eur Heart J, 2018, 39(41): 3701-3711. doi: 10.1093/eurheartj/ehy530
[6] 徐浩, 张治, 解学乾, 等. 冠脉生理功能评估软件(DEEPVESSEL FFR)与有创FFR在评估冠脉缺血中的对比研究[J]. 诊断学理论与实践, 2021, 20(4): 384-390. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDLS202104013.htm
[7] Wang ZQ, Zhou YJ, Zhao YX, et al. Diagnostic accuracy of a deep learning approach to calculate FFR from coronary CT angiography[J]. J Geriatr Cardiol, 2019, 16(1): 42-48.
[8] Eftekhari A, Min J, Achenbach S, et al. Fractional flow reserve derived from coronary computed tomography angiography: diagnostic performance in hypertensive and diabetic patients[J]. Eur Heart J Cardiovasc Imaging, 2017, 18(12): 1351-1360. doi: 10.1093/ehjci/jew209
[9] Zhuang B, Wang S, Zhao S, et al. Computed tomography angiography-derived fractional flow reserve(CT-FFR)for the detection of myocardial ischemia with invasive fractional flow reserve as reference: systematic review and meta-analysis[J]. Eur Radiol, 2020, 30(2): 712-725. doi: 10.1007/s00330-019-06470-8
[10] Ishikawa Y, Akasaka Y, Suzuki K, et al. Anatomic properties of myocardial bridge predisposing to myocardial infarction[J]. Circulation, 2009, 120(5): 376-383. doi: 10.1161/CIRCULATIONAHA.108.820720
[11] 周帆, 闫静, 周长圣, 等. 基于冠状动脉CT血管成像的血流储备分数评估心肌桥血流动力学变化的研究[J]. 中华放射学杂志, 2019, 53(4): 274-280. https://cdmd.cnki.com.cn/Article/CDMD-10284-1019116223.htm
[12] Gao Z, Wang X, Sun S, et al. Learning physical properties in complex visual scenes: An intelligent machine for perceiving blood flow dynamics from static CT angiography imaging[J]. Neural Netw, 2020, 123: 82-93. doi: 10.1016/j.neunet.2019.11.017
[13] 张明多, 南楠, 兰宏志, 等. 基于人工智能优化与计算流体力学的无创血流储备分数对冠状动脉狭窄缺血的诊断价值[J]. 心肺血管病杂志, 2022, 41(3): 243-247. https://www.cnki.com.cn/Article/CJFDTOTAL-XFXZ202203006.htm
[14] Liu X, Wang Y, Zhang H, et al. Evaluation of fractional flow reserve in patients with stable angina: can CT compete with angiography?[J]. Eur Radiol, 2019, 29(7): 3669-3677. doi: 10.1007/s00330-019-06023-z
[15] 褚千琨, 高德宏, 张铭金, 等. RevolutionCT在心肌桥-壁冠状动脉及左心室功能测定的临床应用价值[J]. 现代医用影像学, 2022, 31(3): 402-407. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202203002.htm
[16] Nakanishi R, Rajani R, Ishikawa Y, et al. Myocardial bridging on coronary CTA: an innocent bystander or a culprit in myocardial infarction?[J]. J Cardiovasc Comput Tomogr, 2012, 6(1): 3-13. doi: 10.1016/j.jcct.2011.10.015
[17] 闫玉洁, 袁俊强. 基于CCTA的血流储备分数对心肌桥心肌缺血的评估价值分析[J]. 实验与检验医学, 2021, 39(3): 649-651. doi: 10.3969/j.issn.1674-1129.2021.03.043
[18] 成水华, 倪炯, 刘君, 等. 基于人工智能技术的FFR_(CT)评估左冠状动脉前降支纵深型心肌桥血流动力学变化[J]. 中华医学杂志, 2021, 101(7): 464-469. doi: 10.3760/cma.j.cn112137-20200924-02709
[19] Javadzadegan A, Moshfegh A, Mohammadi M, et al. Haemodynamic impacts of myocardial bridge length: A congenital heart disease[J]. Comput MethodsPrograms Biomed, 2019, 175: 25-33.
[20] 王庭俊, 吴可贵. 病例130: 64岁男性心电图: 异常Q波、ST-T改变[J]. 中华高血压杂志, 2013, 21(3): 291-294. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201303035.htm
[21] 孙淑艳, 张娟. 64排螺旋CT与冠脉造影对心肌桥的对比研究[J]. 包头医学院学报, 2013, 29(2): 47-49. https://www.cnki.com.cn/Article/CJFDTOTAL-BTYX201302024.htm
[22] 杨漠源, 张敏秀, 贾圣琪, 等. 冠状动脉心肌桥合并近端狭窄病变的研究进展[J]. 中国介入心脏病学杂志, 2019, 27(11): 649-652. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXB201911013.htm
[23] Sharzehee M, Chang Y, Song JP, et al. Hemodynamic effects of myocardial bridging in patients with hypertrophic cardiomyopathy[J]. Am J Physiol Heart Circ Physiol, 2019, 317(6): H1282-H1291.
-
图(3)
表(2)
计量
- 文章访问数: 2011
- PDF下载数: 975
- 施引文献: 0