
The predictive value of persistent hypochloremia in the long-term prognosis of heart failure with preserved ejection fraction
-
摘要: 目的 评价持续性低氯血症对射血分数保留型心力衰竭(HFpEF)患者出院1年全因死亡的预测价值。方法 回顾性收集2021年1月—2022年12月于福建省人民医院心血管科出院的HFpEF患者329例,根据患者住院期间平均血氯四分位水平,将患者分为Q1组(平均血氯 < 98.0 mmol/L)、Q2组(98.0 mmol/L≤平均血氯 < 101.5 mmol/L)、Q3组(101.5 mmol/L≤平均血氯 < 104.5 mmol/L)和Q4组(平均血氯≥104.5 mmol/L)。出院后定期门诊或电话随访。采用Kaplan-Meier生存曲线比较各组患者出院1年生存率的差异,Cox回归分析HFpEF患者出院1年全因死亡的危险因素,ROC曲线评估住院期间平均血氯和入院时血氯对HFpEF患者1年死亡的预测价值。结果 Q1、Q2、Q3、Q4组患者出院后1年全因死亡率分别为11.0%、4.9%、3.7%、1.2%(P=0.034)。Kaplan-Meier生存曲线分析显示,持续性低氯血症患者出院1年生存率低于一过性低氯血症患者(P=0.025)。多因素Cox回归分析显示,平均血氯是HFpEF患者随访1年全因死亡的独立危险因素(HR=1.29,95%CI:1.10~1.42,P=0.033)。住院期间平均血氯、入院时血氯预测患者1年全因死亡的ROC曲线下面积分别为0.819、0.698。结论 住院期间平均血氯水平与HFpEF患者1年不良预后相关,其预测HFpEF患者1年预后的价值大于单次的入院时血氯。
-
关键词:
- 心力衰竭, 射血分数保留型 /
- 低氯血症 /
- 预后
Abstract: Objective To evaluate the predictive value of persistent hypochloremia for 1-year all-cause mortality in patients with heart failure with preserved ejection fraction(HFpEF).Methods A total of 329 patients with HFpEF who were discharged from the Department of Cardiology, Fujian Provincial People's Hospital from January 2021 to December 2022 were retrospectively collected. The patients were divided into four groups according to the mean blood chloride quartile level during hospitalization: Q1 group (mean blood chloride < 98.0 mmol/L), Q2 group (98.0 mmol/L≤mean blood chloride < 101.5 mmol/L), Q3 group (101.5 mmol/L≤mean blood chloride < 104.5 mmol/L) and Q4 group (mean blood chloride≥104.5 mmol/L). Regular outpatient or telephone follow-up were conducted after discharge. Kaplan-Meier survival curve was used to compare the 1-year survival rate among the four groups. Cox regression analysis was used to analyze the risk factors of 1-year all-cause death. ROC curve was used to evaluate the predictive value of average blood chlorine during hospitalization and the blood chlorine on admission for 1-year death.Results The 1-year all-cause mortality rates in Q1, Q2, Q3, and Q4 groups after discharge were 11.0%, 4.9%, 3.7%, and 1.2%, respectively. Kaplan-Meier survival curve analysis showed that the 1-year survival rate in discharged patients with persistent hypochloriemia was lower than those with transient hypochloriemia(P=0.025). Multivariate Cox regression analysis showed that the mean blood chloride was an independent risk factor for 1-year all-cause death in HFpEF patients(HR=1.29, 95%CI: 1.10-1.42, P=0.033). The area under the ROC curve of the average blood chlorine during hospitalization and the blood chlorine on admission for predicting 1-year all-cause death were 0.819 and 0.698 respectively.Conclusion The average blood chlorine level during hospitalization is correlated with the 1-year poor prognosis of HFpEF patients, and its predictive value for the 1-year prognosis is greater than the single admission blood chlorine level.-
Key words:
- heart failure with preserved ejection fraction /
- hypochloremia /
- prognosis
-

-
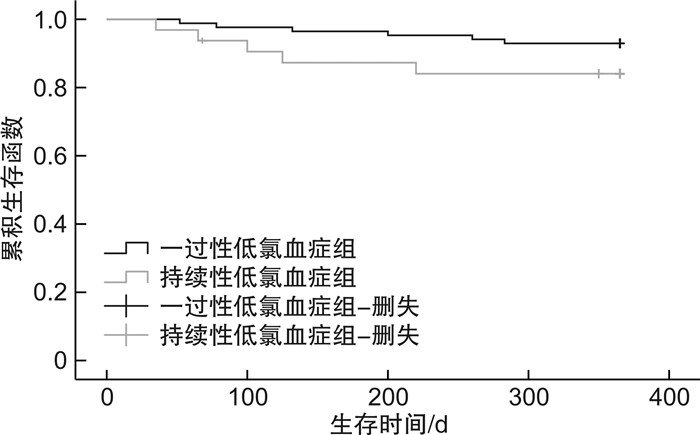
图 1 不同血氯分组HFpEF患者Kaplan-Meier生存曲线
Figure 1. Kaplan-Meier survival curves of HFpEF patients with different blood chlorine
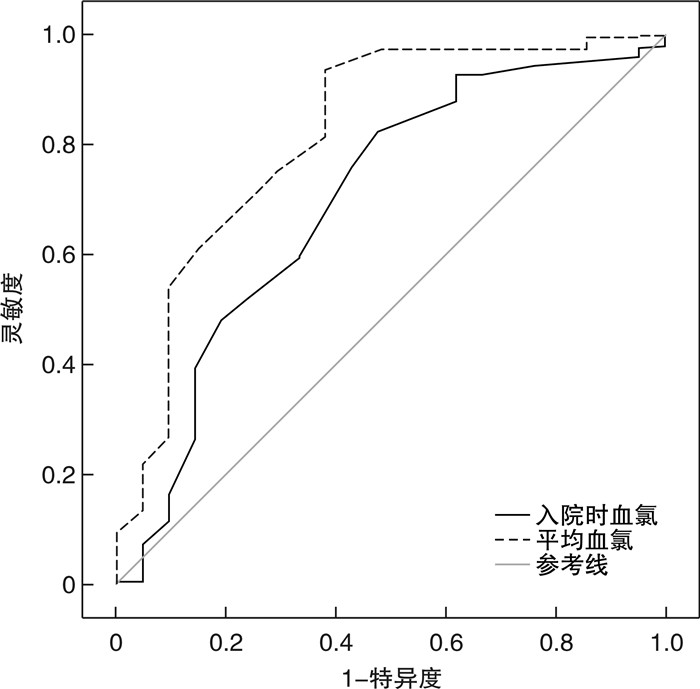
图 2 血氯预测HFpEF患者1年全因死亡的ROC曲线
Figure 2. ROC curves for blood chlorine predicting 1-year all-cause death in HFpEF patients
表 1 患者临床基线特征
Table 1. Clinical baseline data
例(%), X ± S 项目 Q1组(82例) Q2组(82例) Q3组(82例) Q4组(83例) F/χ2 P 年龄/岁 68.31±7.91 68.24±7.71 69.12±7.92 70.23±8.66 3.769 0.088 女性 44(53.7) 37(45.1) 35(42.7) 39(47.0) 2.187 0.535 BMI/(kg/m2) 18.1±3.7 20.9±3.9 22.5±4.3 23.9±4.1 6.235 0.032 冠心病 35(42.7) 30(36.6) 23(28.0) 26(31.3) 4.456 0.216 心肌梗死病史 8(9.8) 6(7.3) 5(6.1) 5(6.0) 1.107 0.775 高血压 44(53.7) 50(61.0) 46(56.1) 51(61.4) 1.459 0.692 糖尿病 30(36.6) 28(34.6) 25(30.5) 24(30.5) 1.414 0.702 心房颤动 25(30.5) 31(37.8) 28(34.1) 20(24.1) 3.915 0.271 入院时 心率/(次/min) 91.06±7.35 90.65±7.22 91.13±7.33 89.75±9.13 3.381 0.120 收缩压/mmHg 112.62±16.31 115.78±17.33 125.32±18.29 130.60±20.30 18.438 < 0.001 血钠/(mmol/L) 130.23±9.01 135.67±9.20 138.46±9.33 140.02±9.75 23.624 < 0.001 血钾/(mmol/L) 3.53±0.41 3.92±0.57 3.61±0.43 3.91±0.55 3.312 0.137 阴离子间隙/(mmol/L) 16.53±1.45 15.73±1.33 14.68±1.27 14.69±138 3.688 0.092 血红蛋白/(g/L) 110.81±13.63 110.23±12.12 112.37±13.05 111.09±12.67 2.347 0.225 血肌酐/(μmol/L) 129.26±34.33 128.39±32.68 125.78±26.82 124.30±27.01 4.745 0.061 NT-proBNP/(pg/mL) 5 567.54±210.23 4 932.51±157.85 3 923.23±159.65 2 558.56±144.25 23.231 < 0.001 NYHAⅢ/Ⅳ级 67(81.7) 58(70.7) 50(61.0) 51(61.4) 10.915 0.012 hs-CRP/(mg/L) 8.23±0.62 7.61±0.58 7.72±0.76 7.83±0.69 3.231 0.167 药物使用 β受体阻滞剂 60(73.2) 65(79.3) 66(80.5) 68(81.9) 2.185 0.535 噻嗪类/襻利尿剂 76(92.7) 69(84.1) 67(81.7) 67(80.7) 5.660 0.129 醛固酮受体拮抗剂 70(85.4) 65(79.3) 64(78.0) 70(84.3) 2.184 0.535 ACEI/ARB/ARNI 73(89.0) 76(92.7) 72(87.8) 75(90.4) 1.109 0.755 SGLT2i 19(23.2) 17(20.7) 14(17.1) 16(19.3) 1.006 0.800 利尿剂抵抗 25(30.5) 19(23.2) 15(18.3) 14(16.9) 5.399 0.145 hs-CRP:超敏C反应蛋白;ACEI:血管紧张素转化酶抑制剂;ARB:血管紧张素受体拮抗剂;ARNI:血管紧张素受体脑啡肽酶抑制剂;SGLT2i:钠-葡萄糖协同转运蛋白2抑制剂。利尿剂抵抗:24 h内静脉应用呋塞米剂量≥80 mg或等同剂量利尿剂后,尿量 < 0.5~1.0 mL/kg/h。  下载: 导出CSV
下载: 导出CSV
表 2 影响HFpEF患者1年全因死亡的多因素Cox回归分析结果
Table 2. Multivariate Cox regression analysis results on 1-year all-cause death in HFpEF patients
因素 β Wald HR 95%CI P 年龄 0.11 15.231 1.14 1.08~1.19 < 0.001 NT-proBNP 1.53 31.382 4.47 3.91~4.92 < 0.001 糖尿病 0.73 9.312 1.89 1.43~3.02 0.012 既往心肌梗死 0.96 10.067 2.42 1.88~4.01 0.008 平均血氯 0.52 5.482 1.29 1.10~1.42 0.033
下载: 导出CSV
-
[1] Misumi K, Matsue Y, Nogi K, et al. Usefulness of incorporating hypochloremia into the get with the guidelines-heart failure risk model in patients with acute heart failure[J]. Am J Cardiol, 2022, 162: 122-128. doi: 10.1016/j.amjcard.2021.09.020
[2] Cuthbert JJ, Pellicori P, Rigby A, et al. Low serum chloride in patients with chronic heart failure: clinical associations and prognostic significance[J]. Eur J Heart Fail, 2018, 20(10): 1426-1435. doi: 10.1002/ejhf.1247
[3] McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J, 2021, 42(36): 3599-3726. doi: 10.1093/eurheartj/ehab368
[4] Kondo T, Yamada T, Tamaki S, et al. Serial Change in Serum Chloride During Hospitalization Could Predict Heart Failure Death in Acute Decompensated Heart Failure Patients[J]. Circ J, 2018, 82(4): 1041-1050. doi: 10.1253/circj.CJ-17-0938
[5] 郭睿康, 池江洋, 严格, 等. 容积调控阴离子通道在心血管疾病中的研究进展[J]. 临床心血管病杂志, 2022, 38(3): 253-257. https://xueshu.baidu.com/usercenter/paper/show?paperid=1c2k0et0ve7e00t03v170040cd027772&site=xueshu_se&hitarticle=1
[6] Zandijk A, van Norel MR, Julius F, et al. Chloride in heart failure: the neglected electrolyte[J]. JACC Heart Fail, 2021, 9(12): 904-915. doi: 10.1016/j.jchf.2021.07.006
[7] Grodin JL, Simon J, Hachamovitch R, et al. Prognostic role of serum chloride levels in acute decompensated heart failure[J]. J Am Coll Cardiol, 2015, 66(6): 659-666. doi: 10.1016/j.jacc.2015.06.007
[8] Kurashima S, Kitai T, Matsue Y, et al. Trajectory of serum chloride levels during decongestive therapy in acute heart failure[J]. Int J Cardiol, 2023, 375: 36-43. doi: 10.1016/j.ijcard.2022.12.041
[9] Bellino MC, Massari F, Albanese M, et al. Baseline and incident hypochloremia in chronic heart failure outpatients: Clinical correlates and prognostic role[J]. Eur J Intern Med, 2021, 84: 32-37. doi: 10.1016/j.ejim.2020.08.021
[10] Hanberg JS, Rao V, Ter Maaten JM, et al. Hypochloremia and diuretic resistance in heart failure: mechanistic insights[J]. Circ Heart Fail, 2016, 9(8): 10.
[11] Griffin M, Soufer A, Goljo E, et al. Real World Use of Hypertonic Saline in Refractory Acute Decompensated Heart Failure: A U.S. Center's Experience[J]. JACC Heart Fail, 2020, 8(3): 199-208. doi: 10.1016/j.jchf.2019.10.012
[12] Kataoka H. The "chloride theory", a unifying hypothesis for renal handling and body fluid distribution in heart failure pathophysiology[J]. Med Hypotheses, 2017, 104: 170-173. doi: 10.1016/j.mehy.2017.06.005
[13] Wu F, Lan Q, Yan L. Prognostic impact of serum chloride concentrations in acute heart failure patients: A systematic Rreview and meta-analysis[J]. Am J Emerg Med, 2023, 71: 109-116. doi: 10.1016/j.ajem.2023.05.035
[14] Shirotani S, Jujo K, Takada T, et al. Renin-angiotensin system inhibitor exerts prognostic effects in HFpEF patients with low baseline chloride level[J]. Int J Cardiol, 2023, 373: 83-89. doi: 10.1016/j.ijcard.2022.11.049
-
图(2)
表(2)
计量
- 文章访问数: 1103
- PDF下载数: 408
- 施引文献: 0