
Construction and validation of a risk-score model for ventricular free wall rupture after acute myocardial infarction
-
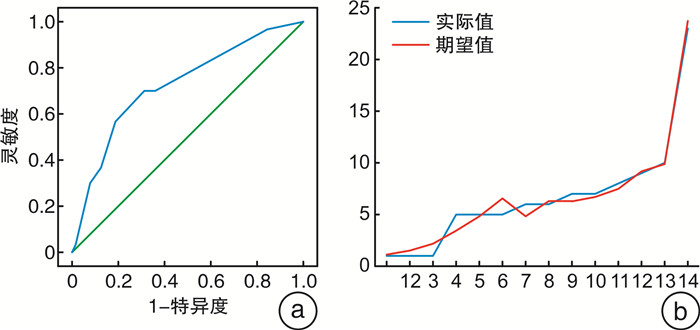
摘要: 目的 构建急性心肌梗死(AMI)患者发生心脏游离壁破裂(FWR)的风险预测评分模型,并对模型进行评价和内部验证。方法 回顾性分析济宁医学院附属医院心内监护室(CCU)2010年1月—2023年8月的233例AMI患者(FWR 73例,非FWR 160例),随机分成建模组139例(FWR 43例,非FWR 96例)和验证组94例(FWR 30例,非FWR 64例)。建模组应用单因素分析和多因素logistic回归分析筛选出FWR的危险因素。根据各危险因素的加权赋分建立FWR风险评分模型,采用受试者工作特征(ROC)曲线下面积(AUC)和Hosmer-Lemeshow检验评估该模型的区分度及校准度,并在验证组中验证该模型价值。结果 建模组中多因素logistic回归分析显示:心包积液(OR=11.478,95%CI:2.881~45.732,P=0.001)、年龄≥62岁(OR=8.930,95%CI:1.539~51.834,P=0.015)、C反应蛋白≥23 mg/L(OR=28.858,95%CI:7.034~118.394,P<0.001)、中性粒细胞百分比≥82%(OR=5.884,95%CI:1.359~25.480,P=0.018)是FWR的独立危险因素。基于这4个危险因素加权赋分建立评分模型,总分9分,评分≤4分划分为低风险,评分≥5分划分为高风险。本研究风险评分模型的AUC为0.924(95%CI:0.879~0.968,P<0.001),Hosmer-Lemeshow检验(χ2=4.110,P=0.847),验证组中AUC为0.725(95%CI:0.613~0.837,P<0.001),Hosmer-Lemeshow检验(χ2=2.368,P=0.796)。结论 本研究建立一种新的简易的风险评分模型,对FWR有良好的预测价值,为临床实践中早期识别AMI后FWR高危患者提供了研究依据。Abstract: Objective To construct a score model for predicting the risk of ventricular free wall rupture (FWR) in patients after acute myocardial infarction (AMI), and to evaluate and detect with independent internal validation.Methods A total of 233 patients with AMI (FWR 73, non-FWR 160) from January 2010 to August 2023 in the Cardiac Care Unit (CCU) of the Affiliated Hospital of Jining Medical College were retrospectively analyzed, and divided into a modeling group of 139 (FWR43, non-FWR96) and a validation group of 94 (FWR30, non-FWR64) randomly. The risk factors of FWR were obtained by univariable and multivariable logistic regression analysis in the modeling group. According to the weighted scores of each independent risk factor, the FWR risk score model was established. The discrimination and calibration of the model were detected by the area under the curve (AUC) of receiver operating characteristic (ROC) and Hosmer-Lemeshow test respectively. The value of the model was examined in the validation group.Results In the modeling grout, the results of the multivariate logistic regression analysis showed that Pericardial effusion (OR=11.478, 95%CI: 2.881-45.732, P=0.001), age≥62 years old (OR=8.930, 95%CI: 1.539-51.834, P=0.015), CRP≥23 mg/L (OR=28.858, 95%CI: 7.034-118.394, P<0.001), neutrophil percentage≥82% (OR=5.884, 95%CI: 1.359-25.480, P=0.018) were independent risk factors for FWR. Based on the weighting of these four risk factors, a scoring model was established with a total score of 9. The patient scores ≤4 were classified as low risk and the scores≥5 were assigned to high risk. In this research, the results of the modeling group with AUC of 0.924 (95%CI: 0.879-0.968, P<0.001) and Hosmer-Lemeshow test (χ2=4.110, P=0.847), while with AUC of 0.725 (95%CI: 0.613-0.837, P<0.001) and Hosmer-Lemeshow test (χ2=2.368, P=0.796) of the internal validation group.Conclusion In this research, a new simple risk score model was established which demonstrated that good predictive value for FWR, and provides a certain reference for early clinical identification of high-risk patients with FWR after AMI.
-

-
表 1 建模组患者临床资料比较
Table 1. Comparison of clinic data of patients of modeling group
例(%), X±S, M(P25, P75) 指标 FWR组(43例) 非FWR组(96例) P值 AUC 女性 18(41.9) 28(29.2) 0.142 年龄/岁 73.14±9.91 66.04±13.72 0.001 0.637 体重指数/(kg/m2) 23.65±3.14 24.80±3.99 0.096 入院时收缩压/mmHg 117.69±24.75 123.28±22.34 0.196 入院时心率/(次/min) 84.18±19.54 76.16±11.86 0.016 0.649 非ST段抬高型心肌梗死 6(13.9) 13(13.5) 0.948 行急诊PCI 15(34.9) 49(51.0) 0.077 高血压史 23(53.5) 51(53.1) 0.968 糖尿病史 11(25.6) 25(26.0) 0.954 脑梗死史 11(25.6) 13(13.5) 0.083 吸烟史 13(30.2) 39(40.6) 0.242 白细胞计数/(×109/L) 11.98±3.90 9.66±3.20 <0.001 0.683 血红蛋白/(g/L) 129.11±17.12 135.52±23.52 0.111 中性粒细胞百分比/% 80.57±9.80 73.99±11.73 0.002 0.679 C反应蛋白/(mg/L) 70.88(28.00,82.99) 3.80(1.85,17.88) <0.001 0.835 白蛋白/(g/L) 35.44±4.87 38.67±4.15 <0.001 0.293 肌酐/(μmol/L) 72.50(52.60,97.90) 64.90(54.85,78.50) 0.247 肌钙蛋白/(ng/mL) 9.507(1.74,30.08) 2.46(0.37,9.00) 0.009 0.665 心脏破裂前心包积液 21(48.8) 14(14.6) <0.001 0.671 射血分数/% 45.13±8.48 47.063±7.86 0.193 左室舒张末期内径/mm 47.88±3.73 47.11±6.05 0.360 室壁瘤 6(13.9) 13(13.5) 0.948 溶栓 2(4.6) 14(14.6) 0.090 β受体阻滞剂 25(58.1) 63(65.6) 0.397 梗死后心绞痛 17(39.5) 20(20.8) 0.021 0.594 注:1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 建模组多因素logistic回归分析结果
Table 2. Results of multivariate logistic regression analysis of modeling group
变量 β P OR 95%CI 赋分 心脏破裂前心包积液 2.440 0.001 11.478 2.881~45.732 2 年龄≥62岁 2.189 0.015 8.930 1.539~51.834 2 C反应蛋白≥23 mg/L 3.362 <0.001 28.858 7.034~118.394 3 中性粒细胞百分比≥82% 1.772 0.018 5.884 1.359~25.480 2 入院心率≥83次/min 0.994 0.115 2.703 0.784~9.325 白细胞≥11.5×109/L 0.131 0.854 1.140 0.281~4.623 肌钙蛋白≥4.4ng/mL 0.657 0.275 1.929 0.593~6.280 梗死后心绞痛 -0.507 0.450 0.602 0.162~2.241 常量 -6.386 <0.001 0.002
下载: 导出CSV
表 3 FWR和非FWR患者CAG比较
Table 3. Comparison of CAG results in FWR and non-FWR patients
例(%) 指标 FWR组(23例) 非FWR组(133例) P值 前降支罪犯血管 10(43.4) 71(53.4) 0.380 回旋支罪犯血管 6(26.1) 13(9.8) 0.027 右冠罪犯血管 5(21.7) 49(36.8) 0.160 单支病变 16(69.6) 60(45.1) 0.030 双支病变 4(17.4) 46(34.6) 0.103 3支病变 3(13.0) 26(19.5) 0.459 罪犯血管次全闭塞 5(21.7) 67(50.4) 0.011
下载: 导出CSV
-
[1] 《中国心血管健康与疾病报告》编写组. 《中国心血管健康与疾病报告2022》要点解读[J]. 中国心血管杂志, 2023, 28(4): 297-312. https://www.cnki.com.cn/Article/CJFDTOTAL-XIXG202304001.htm
[2] 王玉辉, 童路, 帅欣欣. 急性心肌梗死合并游离壁破裂的早期预警[J]. 临床心血管病杂志, 2021, 37(10): 891-895. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2021.10.004
[3] Lanz J, Wyss D, Räber L, et al. Mechanical complications in patients with ST-segment elevation myocardial infarction: A single centre experience[J]. PLOS one, 2019, 14(2): 1-11.
[4] Elbadawi A, Elgendy IY, Mahmoud K, et al. Temporal trends and outcomes of mechanical complications in patients with acute myocardial infarction[J]. JACC Cardiovasc Interv, 2019, 12(18): 1825-1836. doi: 10.1016/j.jcin.2019.04.039
[5] 卢群, 马姗, 宋安齐, 等. 心肌梗死后心脏破裂的现代临床特征和挑战[J]. 中国医学前沿杂志(电子版), 2019, 11(11): 30-40. https://www.cnki.com.cn/Article/CJFDTOTAL-YXQY201911006.htm
[6] 公威, 严研, 聂绍平. 急性心肌梗死合并心脏破裂的诊治研究进展[J]. 中华心血管病杂志, 2022, 50(9): 928-933. doi: 10.3760/cma.j.cn112148-20220610-00458
[7] Xu Z, Li Y, Zhang R, et al. Risk factors for cardiac rupture after acute ST-segment elevation myocardial infarction during the percutaneous coronary intervention era: a retrospective case-control study[J]. J Thorac Dis, 2022, 14(4): 1256-1266. doi: 10.21037/jtd-22-394
[8] Shoji K, Yanishi K, Kawamata H, et al. New risk factors for early-and late-onset cardiac rupture in ST-elevation myocardial infarction patients after primary percutaneous coronary intervention[J]. J Cardiol, 2022, 79(3): 400-407. doi: 10.1016/j.jjcc.2021.10.006
[9] 迪力夏提·吾布力, 田桃, 张兴达, 等. 急性ST段抬高型心肌梗死患者发生心脏破裂的风险预测模型构建及验证[J]. 中国老年学杂志, 2020, 40(3): 449-453. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLXZ202003001.htm
[10] Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction(2018)[J]. J Am Coll Cardiol, 2018, 72(18): 2231-2264. doi: 10.1016/j.jacc.2018.08.1038
[11] 罗雅菲, 戴凯, 李志兵, 等. 急性心肌梗死后心脏破裂的风险预测模型构建与外部验证[J]. 临床心血管病杂志, 2022, 38(2): 107-112. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.02.006
[12] Gong FF, Vaitenas I, Malaisrie SC, et al. Mechanical complications of acute myocardial infarction: a review[J]. JAMA Cardiol, 2021, 6(3): 341-349. doi: 10.1001/jamacardio.2020.3690
[13] 曲红培, 杨杨, 冯喆, 等. 超声在急性心肌梗死后亚急性左室游离壁破裂诊断和预后评估中的应用价值[J]. 中国中西医结合影像学杂志, 2021, 19(5): 440-442. https://www.cnki.com.cn/Article/CJFDTOTAL-JHYX202105009.htm
[14] Oualha D, Ben Abderrahim S, Ben Abdeljelil N, et al. Cardiac rupture during acute myocardial infarction: Autopsy study (2004-2020)[J]. Ann Cardiol Angeiol (Paris), 2023, 72(3): 1-7.
[15] Bittner V. Menopause, age, and cardiovascular risk a complex re lationship[J]. J Am Coll Cardiol, 2009, 54(25): 2374-2375.
[16] Gong W, Li S, Yan Y, et al. Neutrophil counts help predict free wall rupture following st-elevation myocardial infarction[J]. Clin Invest Med, 2021, 44(2): E62-70.
[17] Vasilyev N, Williams T, Brennan ML, et al. Myeloperoxidase-generated oxidants modulate left ventricular remodeling but not infarct size after myocardial infarction[J]. Circulation, 2005, 112: (18): 2812-2820.
[18] Ichihara S, Senbonmatsu T, Price E, et al. Targeted deletion of angiotensin Ⅱ type 2 receptor caused cardiac rupture after acute myocardial infarction[J]. Circulation, 2002, 106(17): 2244-2249.
[19] 李思懿, 公威, 赵冠棋, 等. 急性心肌梗死后心脏破裂临床预测因素研究现状[J]. 中华急诊医学杂志, 2020, 29(3): 437-442.
[20] 马姗, 白玲, 刘平, 等. 联合外周血炎症细胞分类计数和CK-MB对急性心肌梗死后心脏破裂危险性的预测价值[J]. 医学研究生学报, 2021, 34(10): 1045-1051. https://www.cnki.com.cn/Article/CJFDTOTAL-JLYB202110007.htm
[21] Hao W, Lu S, Guo R, et al. Risk factors for cardiac rupture complicating myocardial infarction: a PRISMA meta-analysis and systematic review[J]. J Investig Med, 2019, 67(4): 720-728.
[22] Nozoe M, Sakamoto T, Taguchi E, et al. Clinical manifestation of early phase left ventricular rupture complicating acute myocardial infarction in the primary PCI era[J]. J Cardiol, 2014, 63(1): 14-18.
-

计量
- 文章访问数: 95
- 施引文献: 0