
The association between serum magnesium and vascular endothelial cell secretion function and adverse cardiovascular events in patients with chronic heart failure
-
摘要: 目的 探究血清镁与慢性心力衰竭(CHF)患者血管内皮细胞分泌功能及不良心血管事件(MACE)的关系。方法 选择我院心内科2021年2月—2022年2月住院的266例CHF患者为研究对象。根据随访1年内是否发生MACE,将患者分为MACE组(126例)和无MACE组(140例),比较两组临床资料,采用单因素分析筛选影响MACE发生的因素,通过水平分层回归分析各因素对MACE的作用。采用拆分指标、多元线性回归和限制性立方样条分析MACE发生的独立危险因素及剂量反应关系。构建中介效应模型分析血管内皮细胞分泌功能在血清镁和MACE之间的中介效应。结果 与无MACE组比较,MACE组的血清镁、左心室射血分数(LVEF)、血清钠、收缩压及舒张压显著降低(均P < 0.05),心率、N-末端脑钠肽前体(NT-proBNP)和左心室舒张末期内径显著增加(均P < 0.05),内皮素(ET)、血栓素B2(TXB2)水平显著升高(均P < 0.05),一氧化氮(NO)和6-酮-前列腺素Fla(6-Keto-PGF1α)水平显著降低(均P < 0.05)。拆分指标校正心率、NT-proBNP、ET、TXB2、6-Keto-PGF1α等协变量后,血清镁水平与MACE仍存在独立相关性(OR=0.54,95%CI 0.33~0.76,P < 0.001)。将血清镁转化为二分类变量后,与较高血清镁水平比较,较低的血清镁水平与MACE风险存在独立相关性(OR=0.55,95%CI 0.55~0.91,P < 0.001)。多因素线性回归分析显示,血清镁是预测血管内皮细胞分泌功能的独立因素。LOWESS回归分析显示,血清镁浓度与ET、TXB2、6-Keto-PGF1α浓度呈线性变化。限制性立方样条分析显示,血清镁与MACE存在非线性关系(非线性检验P < 0.001)。构建中介效应模型,发现ET、TXB2和6-Keto-PGF1α均在血清镁和MACE之间发挥部分中介效应。结论 血清镁是MACE发生的独立保护因素,血管内皮细胞分泌功能在血清镁和MACE之间发挥部分中介效应。Abstract: Objective To investigate the relationship between serum magnesium and vascular endothelial cell secretion function and adverse cardiovascular events(MACE) in patients with chronic heart failure (CHF).Methods A total of 266 patients with CHF who were hospitalized in the Department of Cardiology of our hospital from February 2021 to February 2022 were selected as the study subjects, and they were divided into the MACE group (n=126) and non-MACE group (n=140) according to whether MACE occurred within 1 year of follow-up. Clinical data was compared between the two groups. Univariate analysis was used to screen for factors that affect the occurrence of MACE, the effect of each factor on MACE was analyzed by horizontal stratified regression. Split indexes, multiple linear regression, and limiting cubic splines were used to analyze the independent risk factors and dose-response relationship affecting the occurrence of MACE. A mediating effect model was constructed to analyze the mediating effect of vascular endothelial cell secretion function between serum magnesium and MACE.Results Compared with the non-MACE group, the blood magnesium, left ventricular ejection fraction (LVEF), serum sodium, systolic blood pressure, and diastolic blood pressure in the MACE group were significantly reduced (all P < 0.05), heart rate, N-terminal pro-brain natriuretic (NT-proBNP), and left ventricular end-diastolic diameter were significantly increased (all P < 0.05), the levels of endothelin (ET) and thromboxane B2 (TXB2) were significantly increased (both P < 0.05), and the level of 6-keto-prostaglandin Fla (6-Keto-PGF1α) was significantly decreased (P < 0.05). Horizontal stratified regression analysis showed that there was an independent correlation between serum magnesium level and MACE after adjusting for covariates such as heart rate, NT-proBNP, ET, TXB2, and, 6-Keto-PGF1α (OR=0.54, 95%CI 0.33-0.76, P < 0.001). After converting serum magnesium into a dichotomous variable, there was an independent correlation between lower serum magnesium levels and the risk of MACE compared to higher serum magnesium levels (OR=0.55, 95%CI 0.55-0.91, P < 0.001). Multiple linear regression analysis showed that serum magnesium was an independent risk factor for predicting vascular endothelial cell secretion function. LOWESS regression analysis showed that serum magnesium concentration changed linearly with ET, TXB2 and 6-Keto-PGF1α concentrations. Restriction cubic spline analysis showed a nonlinear relationship between serum magnesium and MACE (nonlinear test P < 0.001). The mediating effect model was constructed and it was found that ET, TXB2and 6-Keto-PGF1α all played a partial mediating effect between serum magnesium and MACE.Conclusion Serum magnesium is an independent protective factor for the occurrence of MACE, and vascular endothelial cell secretion plays a partial mediating effect between serum magnesium and MACE.
-

-
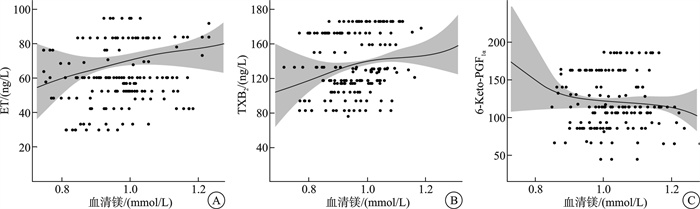
图 1 血清镁浓度与血管内皮细胞分泌功能关系的LOWESS回归分析结果
Figure 1. LOWESS regression analysis of the relationship between serum magnesium concentration and vascular endothelial cell secretion function
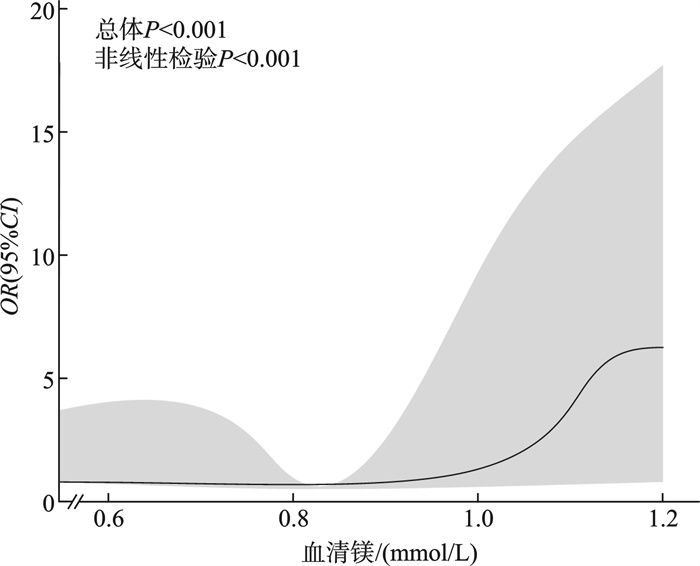
图 2 血清镁与MACE的剂量反应关系
Figure 2. Dose-response relationship between serum magnesium and MACE
表 1 MACE组和无MACE组临床资料比较
Table 1. Comparison of clinical data between the MACE group and non-MACE group
例(%), X±S 项目 MACE组(126例) 无MACE组(140例) χ2/t P 年龄/岁 57.13±15.23 58.62±16.01 0.376 0.708 男性 68(53.96) 88(62.86) 2.161 0.142 BMI 0.217 0.642 ≤24.0 kg/m2 63(50.0) 74(52.86) >24.0 kg/m2 63(50.0) 66(47.14) 血清镁 150.117 < 0.001 ≤0.84 mmol/L 107(84.92) 14(10.0) >0.84 mmol/L 19(15.08) 126(90.0) 高血压 53(42.06) 49(35.00) 1.400 0.237 糖尿病 49(38.89) 42(30.00) 2.328 0.127 冠心病 58(46.03) 56(40.00) 0.985 0.321 扩心病 39(30.95) 35(25.00) 1.170 0.279 吸烟 63(50.0) 67(47.86) 0.122 0.727 饮酒 78(61.90) 77(55.0) 1.300 0.254 LVEF/% 42.72±3.27 58.26±4.09 16.273 0.001 发生心律失常 46(36.51) 37(26.51) 3.138 0.076 收缩压/mmHg 105.27±13.27 119.37±15.21 3.865 0.001 舒张压/mmHg 69.22±14.27 78.18±11.36 2.828 0.006 心率/(次/min) 95.71±17.18 75.82±15.48 4.884 0.001 血清钾/(mmol/L) 4.42±0.42 4.26±0.35 1.676 0.098 血清钠/(mmol/L) 130.32±1.65 139.91±1.38 25.527 0.001 抗心力衰竭药物使用 0.073 0.787 利尿剂 38(30.16) 35(25.00) β受体阻滞剂 53(42.06) 53(37.86) ACEI/ARB 35(27.78) 52(37.14) 血肌酐/(μmol/L) 103.40±36.21 99.34±38.79 0.880 0.380 ALT/(U/L) 54.26±5.21 52.39±5.04 1.482 0.143 AST/(U/L) 40.71±4.72 39.64±4.66 0.927 0.358 HDL-C/(mmol/L) 1.12±0.43 0.98±0.32 1.500 0.138 LDL-C/(mmol/L) 4.19±1.03 3.99±0.94 0.824 0.413 NT-proBNP/(ng/L) 1 365.52±112.74 946.18±81.32 35.036 < 0.001 LVEDD/mm 61.05±12.83 40.29±14.39 5.971 < 0.001 注:1 mmHg=0.133 kPa;ACEI:血管紧张素转化酶抑制剂;ARB:血管紧张素受体阻滞剂。  下载: 导出CSV
下载: 导出CSV
表 2 MACE组和无MACE组血管内皮细胞分泌功能比较
Table 2. Comparison of vascular endothelial cell secretory function between the two groups
X±S 项目 MACE组(126例) 无MACE组(140例) t P ET/(ng/L) 60.37±5.28 50.28±3.96 8.858 0.001 NO/(μmol/L) 63.59±6.82 69.23±7.25 3.255 0.002 TXB2/(ng/L) 148.28±10.38 124.12±9.29 9.856 0.001 6-Keto-PGF1α/(ng/L) 120.75±7.86 137.63±4.96 10.713 0.001
下载: 导出CSV
表 3 血清镁与MACE的独立相关性
Table 3. Independent association of serum magnesium with MACE
OR(95%CI) 变量 未校正模型 模型1 模型2 模型3 模型4 模型5 血清镁 0.51
(0.40~0.80)0.58
(0.37~0.78)0.55
(0.32~0.68)0.50
(0.28~0.65)0.53
(0.38~0.69)0.54
(0.33~0.76)血清镁二分类 高血清镁水平 1 1 1 1 1 1 低血清镁水平 0.75
(0.54~0.98)0.77
(0.50~0.91)0.78
(0.51~0.97)0.81
(0.56~0.93)0.76
(0.49~0.99)0.82
(0.55~0.91)血清镁五分位数组 Q1 1 1 1 1 1 1 Q2 0.77
(0.52~0.96)0.76
(0.50~0.94)0.81
(0.49~0.90)0.79
(0.55~0.93)0.75
(0.56~0.95)0.81
(0.52~0.90)Q3 0.71
(0.49~0.88)0.72
(0.45~0.86)0.75
(0.44~0.84)0.72
(0.48~0.89)0.68
(0.41~0.83)0.74
(0.46~0.89)Q4 0.65
(0.39~0.81)0.61
(0.43~0.79)0.69
(0.39~0.77)0.65
(0.40~0.81)0.60
(0.38~0.73)0.70
(0.39~0.80)Q5 0.50
(0.38~0.72)0.54
(0.41~0.73)0.52
(0.37~0.77)0.49
(0.40~0.7100.46
(0.44~0.70)0.48
(0.41~0.69)P趋势 0.003 0.001 < 0.001 0.001 0.001 < 0.001 模型1:调整心率;模型2:调整心率、NT-proBNP;模型3:调整心率、NT-proBNP、ET;模型4:调整心率、NT-proBNP、ET、TXB2;模型5:调整心率、NT-proBNP、ET、TXB2、6-Keto-PGF1α。高血清镁水平:>0.84 mmol/L;低血清镁水平:≤0.84 mmol/L;Q1:≥0.84 mmol/L;Q2:≥0.75 mmol/L且 < 0.84 mmol/L;Q3:≥0.65 mmol/L且 < 0.75 mmol/L;Q4:≥0.55 mmol/L且 < 0.65 mmol/L;Q5: < 0.55 mmol/L。
下载: 导出CSV
表 4 血清镁与血管内皮细胞分泌功能的多因素线性回归分析
Table 4. Multiple linear regression analysis of serum magnesium and vascular endothelial cell secretion function
项目 未校正模型 模型1 模型2 β(95%CI) P β(95%CI) P β(95%CI) P ET 23.29(19.07~37.83) < 0.001 16.37(9.10~29.08) 0.032 15.83(10.43~26.93) 0.019 TXB2 20.64(19.36~31.37) < 0.001 18.36(16.96~29.74) 0.025 16.75(12.28~23.86) 0.021 6-Keto-PGF1α -21.03(-33.36~ -20.01) < 0.001 -18.92(-28.36~ -17.38) 0.037 -16.93(-25.86~ -13.90) 0.015 模型1:校正后的LVEF、收缩压、舒张压、血清钠、NT-proBNP、心率、LVEDD;模型2:校正后的模型1,ET、TXB2、6-Keto-PGF1α。
下载: 导出CSV
表 5 MACE与血清镁剂量的关系
Table 5. Relationship between MACE and serum magnesium dose
模型 P 模型Ⅰ 标准线性效应 1.081(1.022~1.095) < 0.001 模型Ⅱ 血清镁的拐点 0.84 血清镁 < 0.84 mmol/L 0.999(0.901~1.085) < 0.001 血清镁≥ 0.84 mmol/L 1.011(1.003~1.020) < 0.001 效应差 1.025(1.013~1.034) < 0.001 对数似然比检验 < 0.001
下载: 导出CSV
表 6 血管内皮细胞分泌功能对血清镁和MACE的中介效应模型
Table 6. Model of mediating effect of vascular endothelial cell secretion on serum magnesium and MACE
因变量 自变量 β SE t值 P值 模型1 MACE 血清镁 0.256 0.45 6.389 < 0.001 模型2 ET 血清镁 0.341 0.47 7.392 < 0.001 TXB2 血清镁 0.239 0.56 4.284 < 0.001 6-Keto-PGF1α 血清镁 0.201 0.45 5.297 < 0.001 模型3 MACE 血清镁 0.160 0.48 3.394 < 0.001 ET 0.357 0.46 7.392 < 0.001 MACE 血清镁 0.152 0.53 2.936 < 0.001 TXB2 0.276 0.55 4.826 < 0.001 MACE 血清镁 0.376 0.48 3.027 < 0.001 6-Keto-PGF1α 0.322 0.44 5.826 < 0.001 模型1:血清镁预测MACE;模型2:血清镁预测血管内皮细胞分泌功能;模型3:血清镁和血管内皮细胞分泌功能共同预测MACE。
下载: 导出CSV
-
[1] Sun Z, Wang Z, Yun Z, et al. Machine learning-based model for worsening heart failure risk in Chinese chronic heart failure patients[J]. ESC Heart Fail, 2025, 12(1): 211-228. doi: 10.1002/ehf2.15066
[2] 赵灿, 王刚, 刘霄燕, 等. BMI对慢性心力衰竭的预后价值[J]. 临床心血管病杂志, 2024, 40(3): 194-198. doi: 10.13201/j.issn.1001-1439.2024.03.007
[3] 李春霞, 卜星彭, 李丽, 等. 老年慢性心力衰竭风险评估临床应用及心血管不良事件危险因素的预测分析[J]. 中华老年心脑血管病杂志, 2022, 24(8): 815-819.
[4] 贾婉茹, 项欣, 王璐, 等. 慢性心力衰竭患者临床特征及心血管不良事件的危险因素分析[J]. 中国循证心血管医学杂志, 2024, 16(3): 304-306.
[5] 刘占军, 马利军, 郑莹莹. 外周血单个核细胞TFAM、GDF-15、淋巴细胞β1-AR的mRNA对近期MACE的预测效能[J]. 医学分子生物学杂志, 2021, 18(6): 461-467.
[6] 张国天, 杨建峰, 颜文华, 等. 血清钠、钾水平变异性与慢性心力衰竭病人不良心血管事件的关系[J]. 中西医结合心脑血管病杂志, 2023, 21(5): 870-873.
[7] Gori M, Claggett B, Senni M, et al. Combining diastolic dysfunction and natriuretic peptides to risk stratify patients with heart failure with reduced ejection fraction[J]. Int J Cardiol, 2021, 335: 59-65. http://www.zhangqiaokeyan.com/journal-foreign-detail/0704029490080.html
[8] 高乃婧, 汤海华, 陈怡, 等. S100A12在预测慢性心力衰竭患者不良临床终点事件中的意义[J]. 临床急诊杂志, 2022, 23(9): 655-659.
[9] McDonagh TA, Metra M, Adamo M, et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J, 2023, 44(37): 3627-3639.
[10] Coiro S, Girerd N, McMurray JJV, et al. Diuretic therapy as prognostic enrichment factor for clinical trials in patients with heart failure with reduced ejection fraction[J]. Clin Res Cardiol, 2021, 110(8): 1308-1320.
[11] 陈红, 赵敬东, 李兴升. 老年慢性心力衰竭恶化的风险模型构建及NT-proBNP的预测价值探讨[J]. 临床心血管病杂志, 2024, 40(3): 199-206. doi: 10.13201/j.issn.1001-1439.2024.03.008
[12] Saito Y, Tanaka A, Node K, et al. Uric acid and cardiovascular disease: a clinical review[J]. J Cardiol, 2021, 78(1): 51-57. http://www.sciencedirect.com/science/article/pii/S0914508720304159
[13] Kim OK, Kim K, Park S, et al. Clinical relevance of serum ionized magnesium concentration in dogs with myxomatous mitral valve disease[J]. J Vet Intern Med, 2024, 38(1): 41-50. http://openurl.ebsco.com/contentitem/doi:10.1111%2Fjvim.16963?sid=ebsco:plink:crawler&id=ebsco:doi:10.1111%2Fjvim.16963
[14] Mondellini GM, Verbrugge FH. Evaluation and Management of Hyponatremia in Heart Failure[J]. Curr Heart Fail Rep, 2024, 21(3): 252-261. http://www.ncbi.nlm.nih.gov/pubmed/38411885
[15] 李亮, 罗艺, 沈磊, 等. 心脏磁共振T1 mapping评价缺血性心肌病心肌纤维化与LVEF及NT-proBNP的关系[J]. 中国医学计算机成像杂志, 2021, 27(1): 10-15.
[16] 袁小惠, 桑卓, 庄雯雯. 血清镁水平与左心室射血分数保留的心力衰竭老年患者心脏结构及预后的关系[J]. 心脑血管病防治, 2023, 23(3): 57-60.
[17] Cunningham JW, Myhre PL. NT-proBNP response to heart failure therapies: an imperfect surrogate[J]. J Am Coll Cardiol, 2021, 78(13): 1333-1336.
[18] Moreno-González R, Formiga F, Mora Lujan JM, et al. Usefulness of systolic blood pressure combined with heart rate measured on admission to identify 1-year all-cause mortality risk in elderly patients firstly hospitalized due to acute heart failure[J]. Aging Clin Exp Res, 2020, 32(1): 99-106. http://pubmed.ncbi.nlm.nih.gov/30790241/
[19] 和紫铉, 田晶, 韩港飞, 等. 慢性心力衰竭患者住院期间血压水平及变化对全因死亡的影响[J]. 中华高血压杂志, 2024, 32(1): 57-64.
[20] 努尔比牙·吾买尔, 郭玉君, 姑丽努尔·麦麦提吐尔逊, 等. 血清Na+水平对慢性心力衰竭患者预后的预测价值[J]. 新疆医科大学学报, 2023, 46(6): 751-758.
[21] 张亚琴, 李艳婷, 单丹丹, 等. 协同护理模式在全髋关节置换术后恐动症患者中的应用[J]. 中华护理杂志, 2021, 56(4): 515-520.
[22] 罗文宽, 卢健棋, 潘朝锌, 等. 基于改善血管内皮功能的角度探讨中医药防治心力衰竭[J]. 中西医结合心脑血管病杂志, 2024, 22(12): 2169-2174.
[23] 马蓉, 赵蓓. 硝苯地平联合硫酸镁对妊高症患者子宫动脉血流动力学、血管内皮功能及母婴结局的影响[J]. 贵州医药, 2024, 48(8): 1250-1252.
[24] 李姝, 仝玉珠, 李平平. 镇肝熄风汤对子痫前期患者钙镁离子水平、细胞毒性因子-血管内皮功能的影响[J]. 世界中西医结合杂志, 2023, 18(4): 728-732, 736.
[25] 崔菲, 王敏, 王春花, 等. 镁的内稳态及其与心血管疾病相关性的研究进展[J]. 中国当代医药, 2023, 30(6): 33-38, 43.
-
计量
- 文章访问数: 305
- 施引文献: 0