
Development and evaluation of a nomogram for incident atrial fibrillation based on national basic public health service project
-
摘要: 目的 面向基层重点监测人群(老年人、高血压患者和糖尿病患者),构建简易、可靠的新发心房颤动(房颤)风险预警模型。方法 纳入2015年1月—2020年12月在广州市增城区新塘镇参与国家基本公共卫生服务项目年度体检的8443例受试者,将其按照2∶1的比例随机分配至建模组和验证组,随后建模组将按照随访期间是否新发房颤分为无房颤组和新发房颤组。将两组基线差异变量经Stepwise筛选后,得出模型最终变量,并构建风险列线图。结果 本研究构建的风险预警模型包含3个极易获取的变量(年龄、舒张压、BMI)。无论在建模组还是验证组,该列线图的3、4、5年AUC均达到了0.7以上,校准曲线也体现了良好的一致性。结论 本研究构建的风险预警模型可有效面向基层重点监测人群识别新发房颤高危患者。Abstract: Objective To develop a simple and reliable prediction model for incident atrial fibrillation(AF) for intensive monitoring population(elderly, hypertensive patients and diabetic patients) in primary care.Methods The 8443 enrolled subjects who participated were randomly(2: 1) assigned to the development cohort and the validation cohort in the annual physical examination of the National Basic Public Health Service Project in Xintang, Zengcheng District, Guangzhou from January 2015 to December 2020. Then patients in the development cohort will be further divided into non-AF group and AF group based on whether they developed AF during the follow-up period. Variables that were unbalanced between groups will be screened through a stepwise approach. And, based on the filtered variables, a prediction model was constructed.Results The prediction model constructed in this study contains only 3 easily accessible variables(age, diastolic blood pressure, body mass index). Either in the development cohort or the validation cohort, the 3-, 4-, and 5-year AUC of the nomogram reached 0.7 or more, and the calibration curve also demonstrated good consistency.Conclusion Our prediction model can effectively identify at-risk patients of incident AF among intensive monitoring population in primary care setting.
-
Key words:
- atrial fibrillation /
- prediction model /
- nomogram /
- primary prevention
-

-
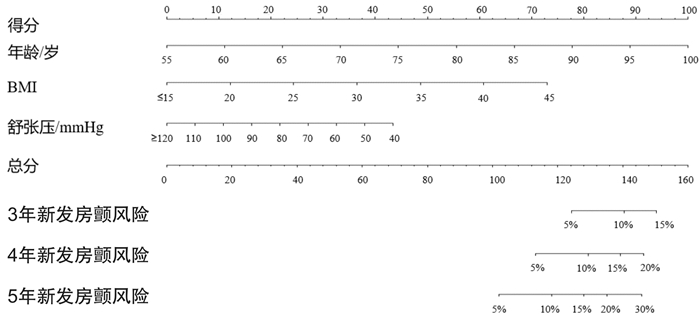
图 1 新发房颤的风险列线图
Figure 1. Nomogram to estimate the risk of incident atrial fibrillation

图 2 新发房颤风险列线图的3、4、5年时间依赖ROC曲线
Figure 2. The 3, 4, 5 years time-dependent receiver operator characteristic curves of the nomogram forincident atrial fibrillation
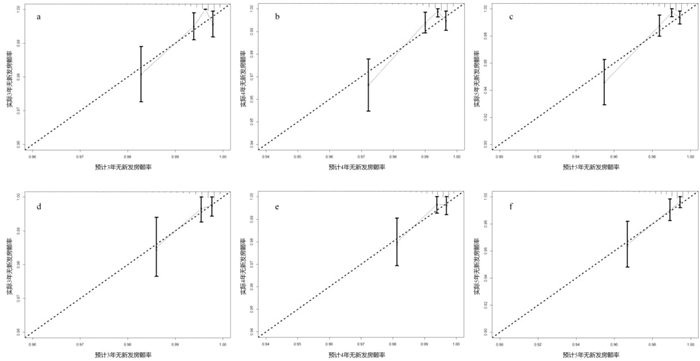
图 3 新发房颤风险列线图的3、4、5年校准曲线
Figure 3. The 3, 4, 5 years calibrationplots of the nomogram forincident atrial fibrillation
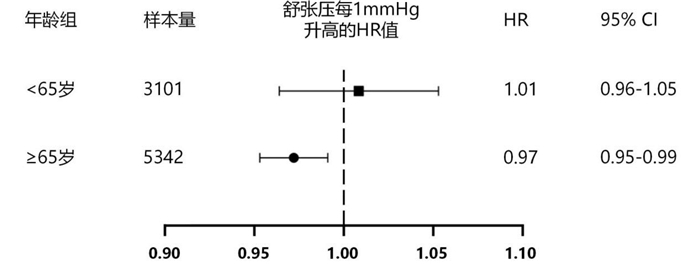
图 4 舒张压在老年人或非老年人中与新发房颤的关系
Figure 4. Adjusted hazard ratio of 1 mmHg higher DBP for incident atrial fibrillation stratified by age subgroup
表 1 建模组无房颤组与新发房颤组基线资料比较
Table 1. Comparison of baseline characteristics between non-AF group and AF group in the development cohort
X±S, M(P25, P75), 例(%) 变量 无房颤组(5550例) 新发房颤组(70例) t/Z/χ2值 P值 年龄/岁 67.70 ± 6.79 72.13 ± 6.99 -5.419 < 0.001 男性 2143(38.61) 24(34.29) 0.546 0.460 高血压 2873(52.80) 49(70.00) 8.224 0.004 糖尿病 992(17.87) 13(18.57) 0.023 0.880 心率/(次·min-1) 78.13 ± 12.24 75.94 ± 12.89 1.484 0.138 收缩压/mmHg 146.37±20.27 148.11 ± 20.59 -0.715 0.475 舒张压/mmHg 81.82± 11.26 78.00 ± 11.81 2.818 0.005 BMI/(kg·m-2) 24.44 ± 3.63 25.76 ± 4.11 -3.010 0.003 腰围/cm 85.05 ± 9.42 88.16 ± 11.44 -2.735 0.006 吸烟 5.833 0.050 从不 4536(81.76) 65(92.86) 已戒烟 310(5.59) 2(2.86) 正在吸烟 702(12.65) 3(4.29) 饮酒频率 0.188 1.000 从不 4896(88.22) 63(90.00) 有时 481(8.67) 6(8.57) 经常 75(1.35) 0(0.00) 每天 98(1.77) 1(1.43) 运动频率 0.825 0.839 从不 2566(46.27) 32(46.38) 偶尔 847(15.27) 13(18.84) 每周至少一次 285(5.14) 3(4.35) 每天 1848(33.32) 21(30.43) 空腹血糖/(mmol·L-1) 4.88(4.41,5.52) 4.88(4.46,5.64) -0.605 0.545 血红蛋白/(g·L-1) 136.00(127.00,145.00) 135.50(127.00,145.75) -0.218 0.827 肌酐/(μmol·L-1) 65.90(54.80,80.60) 68.95(57.75,78.23) -0.531 0.596 总胆固醇/(mmol·L-1) 5.34(4.60,6.08) 5.10(4.29,5.60) -2.645 0.008 甘油三酯/(mmol·L-1) 1.43(0.99,2.10) 1.51(1.04,1.83) -0.144 0.885  下载: 导出CSV
下载: 导出CSV
表 2 新发房颤危险因素的单因素及多因素Cox比例风险回归模型
Table 2. Univariable and multivariable Cox proportional hazard regression for risk factors of incident atrial fibrillation.
变量 单因素回归分析 多因素回归分析 HR(95%CI) P值 HR(95%CI) P值 年龄 1.10(1.07~1.14) < 0.001 1.10(1.07~1.14) < 0.001 BMI 1.09(1.02~1.15) 0.006 1.11(1.05~1.18) < 0.001 高血压 2.06(1.24~3.43) 0.006 舒张压 0.97(0.95~0.99) 0.004 0.98(0.96~1.00) 0.030 腰围 1.04(1.01~1.06) 0.004 总胆固醇 0.98(0.77~1.24) 0.864
下载: 导出CSV
-
[1] Ruddox V, Sandven I, Munkhaugen J, et al. Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure: A systematic review and meta-analysis[J]. Eur J Prev Cardiol, 2017, 24(14): 1555-1566. doi: 10.1177/2047487317715769
[2] Gómez-Outes A, Lagunar-Ruíz J, Terleira-Fernández AI, et al. Causes of death in anticoagulated patients with atrial fibrillation[J]. J Am Coll Cardiol, 2016, 68(23): 2508-2521. doi: 10.1016/j.jacc.2016.09.944
[3] 陈楚云, 杨颖, 张岩. 心房衰竭: 新的临床综合征?[J]. 临床心血管病杂志, 2021, 37(10): 882-886. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202110002.htm
[4] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2020概要[J]. 中国循环杂志, 2021, 36(6): 521-545. doi: 10.3969/j.issn.1000-3614.2021.06.001
[5] Lowres N, Neubeck L, Redfern J, et al. Screening to identify unknown atrial fibrillation. A systematic review[J]. Thromb Haemost, 2013, 110(2): 213-222. doi: 10.1160/TH13-02-0165
[6] Kirchhof P. The future of atrial fibrillation management: integrated care and stratified therapy[J]. Lancet, 2017, 390(10105): 1873-1887. doi: 10.1016/S0140-6736(17)31072-3
[7] Keach JW, Bradley SM, Turakhia MP, et al. Early detection of occult atrial fibrillation and stroke prevention[J]. Heart, 2015, 101(14): 1097-1102. doi: 10.1136/heartjnl-2015-307588
[8] Schnabel RB, Sullivan LM, Levy D, et al. Development of a risk score for atrial fibrillation(Framingham Heart Study): a community-based cohort study[J]. Lancet, 2009, 373(9665): 739-745. doi: 10.1016/S0140-6736(09)60443-8
[9] Yang P, Zhao Y, Wong ND. Development of a risk score for atrial fibrillation in adults with diabetes mellitus(from the ACCORD Study)[J]. Am J Cardiol, 2020, 125(11): 1638-1643. doi: 10.1016/j.amjcard.2020.03.002
[10] Kokubo Y, Watanabe M, Higashiyama A, et al. Development of a basic risk score for incident atrial fibrillation in a japanese general population-the suita study[J]. Circ J, 2017, 81(11): 1580-1588. doi: 10.1253/circj.CJ-17-0277
[11] Li YG, Pastori D, Farcomeni A, et al. A Simple clinical risk score(C(2) HEST)for predicting incident atrial fibrillation in asian subjects: derivation in 471, 446 Chinese subjects, with internal validation and external application in 451, 199 Korean subjects[J]. Chest, 2019, 155(3): 510-518. doi: 10.1016/j.chest.2018.09.011
[12] 李延广. 新发心房颤动风险评估模型的建立、验证与应用[D]. 中国人民解放军医学院, 2019.
[13] Li S, Cheng J, Cui L, et al. Cohort study of repeated measurements of serum urate and risk of incident atrial fibrillation[J]. J Am Heart Assoc, 2019, 8(13): e12020.
[14] Wang TJ, Parise H, Levy D, et al. Obesity and the risk of new-onset atrial fibrillation[J]. JAMA, 2004, 292(20): 2471-2477. doi: 10.1001/jama.292.20.2471
[15] Macfarlane PW, Murray H, Sattar N, et al. The incidence and risk factors for new onset atrial fibrillation in the PROSPER study[J]. Europace, 2011, 13(5): 634-639. doi: 10.1093/europace/eur016
[16] Emdin CA, Anderson SG, Salimi-Khorshidi G, et al. Usual blood pressure, atrial fibrillation and vascular risk: evidence from 4.3 million adults[J]. Int J Epidemiol, 2017, 46(1): 162-172.
[17] Chang TI, Liu S, Airy M, et al. Blood pressure and incident atrial fibrillation in older patients initiating hemodialysis[J]. Clin J Am Soc Nephrol, 2019, 14(7): 1029-1038. doi: 10.2215/CJN.13511118
[18] 伏蕊, 窦克非, 许海燕, 等. 中国非ST段抬高型心肌梗死患者随访24个月期间死亡的独立危险因素分析[J]. 中国循环杂志, 2020, 35(10): 985-989. doi: 10.3969/j.issn.1000-3614.2020.10.008
[19] Guichard JL, Desai RV, Ahmed MI, et al. Isolated diastolic hypotension and incident heart failure in older adults[J]. Hypertension, 2011, 58(5): 895-901. doi: 10.1161/HYPERTENSIONAHA.111.178178
[20] Protogerou AD, Safar ME, Iaria P, et al. Diastolic blood pressure and mortality in the elderly with cardiovascular disease[J]. Hypertension, 2007, 50(1): 172-180. doi: 10.1161/HYPERTENSIONAHA.107.089797
[21] Wu X, Chen M, Wang K, et al. Gender differences in prognostic markers of all-cause death in patients with acute heart failure: a prospective 18-month follow-up study[J]. J Cardiovasc Transl Res, 2020, 13(1): 97-109. doi: 10.1007/s12265-019-09893-2
[22] Curry SJ, Krist AH, Owens DK, et al. Screening for atrial fibrillation with electrocardiography: US preventive services task force recommendation statement[J]. JAMA. 2018, 320(5): 478-484. doi: 10.1001/jama.2018.10321
[23] Jones NR, Taylor CJ, Hobbs F, et al. Screening for atrial fibrillation: a call for evidence[J]. Eur Heart J, 2020, 41(10): 1075-1085. doi: 10.1093/eurheartj/ehz834
-
图(4)
表(2)
计量
- 文章访问数: 1718
- PDF下载数: 961
- 施引文献: 0