
The value of serum YKL-40 combined with CHA2DS2-VASc-HSF score in the diagnosis of acute ST-segment elevation myocardial infarction
-
摘要: 目的 探讨血清几丁质酶3样蛋白1(YKL-40)和CHA2DS2-VASc-HSF评分在急性ST段抬高型心肌梗死(STEMI)诊断中的价值。方法 选取2020年12月—2022年1月合肥市第二人民医院广德路院区胸痛中心收治的STEMI患者为STEMI组(85例),同期因胸痛就诊冠状动脉(冠脉)造影检查阴性患者为对照组(81例),检测2组血清YKL-40浓度。同时,收集患者一般临床资料计算CHA2DS2-VASc-HSF评分。Pearson相关分析STEMI患者血清YKL-40、CHA2DS2-VASc-HSF评分与cTnI的相关性;应用多因素logistic回归分析筛选STEMI独立危险因素;受试者工作特征曲线(ROC)评价血清YKL-40水平、CHA2DS2-VASc-HSF评分在STEMI诊断中的价值。结果 STEMI组患者血清YKL-40水平为(1116.82±608.15) ng/dL,对照组血清YKL-40水平为(737.65±449.66) ng/dL,差异有统计学意义(P< 0.05)。STEMI组患者CHA2DS2-VASc-HSF评分为(4.34±2.14)分,对照组CHA2DS2-VASc-HSF评分为(3.19±1.4)分,差异有统计学意义(P< 0.05)。Pearson相关分析显示,STEMI患者血清YKL-40、CHA2DS2-VASc-HSF评分与cTnI水平呈明显正相关(r=0.382,P< 0.001;r=0.293,P=0.007)。多因素logistic回归分析显示,血清YKL-40、CHA2DS2-VASc-HSF评分、白细胞及空腹血糖为发生STEMI的独立危险因素(P< 0.05)。ROC分析结果显示,血清YKL-40预测STEMI发生的曲线下面积(AUC)为0.687(95%CI:0.607~0.767,P< 0.001),灵敏度为0.553,特异度为0.753,最佳截断值为960.73 ng/dL。CHA2DS2-VASc-HSF评分预测STEMI发生的AUC为0.654(95%CI:0.572~0.736,P=0.001),灵敏度为0.235,特异度为0.975,最佳截断值为5.5。血清YKL-40联合CHA2DS2-VASc-HSF评分预测STEMI发生的AUC为0.741(95%CI:0.668~0.815,P< 0.001),灵敏度为0.624,特异度为0.765。结论 血清YKL-40、CHA2DS2-VASc-HSF评分均与STEMI的发生相关,两项联合检测对STEMI诊断具有较高价值。
-
关键词:
- 急性ST段抬高型心肌梗死 /
- 血清几丁质酶3样蛋白1 /
- CHA2DS2-VASc-HSF评分 /
- 诊断价值
Abstract: Objective To investigate the value of serum YKL-40 combined with CHA2DS2-VASc-HSFscore in the diagnosis of acute st-segment elevation myocardial infarction(STEMI).Methods Patients with STEMI(85 cases) admitted to the chest pain center of Guangde Road Hospital, Second People's Hospital of Hefei from December 2020 to January 2022 were selected. The patients with negative coronary angiography in our hospital during the same period were the control group(81 cases), and the serum YKL-40 concentration in the two groups was detected. Meanwhile, general clinical data of patients were collected to calculate CHA2DS2-VASc-HSFscores. Pearson correlation analysis was performed to analyze the correlation between serum YKL-40, CHA2DS2-VASc-HSF scores and cTnI in STEMI patients; Multi-factor logistic regression analysis was applied to screen independent risk factors for STEMI; The subject operating characteristic curve(ROC) was used to evaluate the value of serum YKL-40 level and CHA2DS2-VASc-HSF scores in the diagnosis of STEMI.Results The serum YKL-40 level was(1116.82±608.15) ng/dL in the STEMI group patients and(737.65±449.66) ng/dL in the control group, with statistically significant differences(P< 0.001). The CHA2DS2-VASc-HSF score of patients in the STEMI group was(4.34±2.14) score and the B score of the control group was(3.19±1.4) score, and the difference was statistically significant(P< 0.001). Pearson correlation analysis showed a significant positive correlation between serum YKL-40, CHA2DS2-VASc-HSF scores and cTnI levels in STEMI patients(r=0.382,P< 0.001;r=0.293,P=0.007). Multi-factor logistic regression analysis showed that serum YKL-40 CHA2DS2-VASc-HSF scores, leukocytes, and fasting glucose were independent risk factors for the development of STEMI(P< 0.05). ROC analysis showed that the area under the curve(AUC) of serum YKL-40 predicted the occurrence of STEMI was 0.687(95%CI: 0.607-0.767,P< 0.001), with a sensitivity of 0.553 and specificity of 0.753, and the best cut-off value was 960.73 ng/dL.The CHA2DS2-VASc-HSF score predicted that the area under the curve(AUC) for the occurrence of STEMI was 0.654(95%CI: 0.572-0.736,P=0.001), the sensitivity was 0.235, the specificity was 0.975, and the optimal cut-off value was 5.5. The area under the curve(AUC) of serum YKL-40 combined with the CHA2DS2-VASc-HSF score for predicting STEMI occurrence was 0.741(95%CI: 0.668-0.815,P< 0.001), with a sensitivity of 0.624 and a specificity of 0.765.Conclusion Serum YKL-40 and CHA2DS2-VASc-HSF score are correlated with the occurrence of STEMI, and the two combined tests were of high value for STEMI diagnosis. -

-
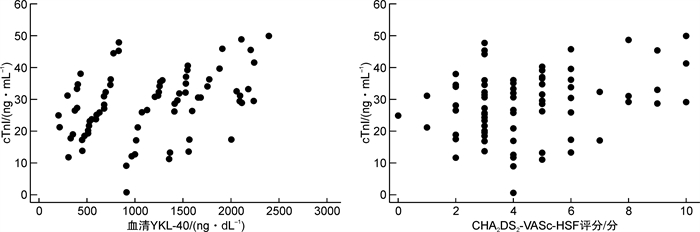
图 1 血清YKL-40、CHA2DS2-VASc-HSF评分与cTnI相关性分析
Figure 1. Correlation analysis between serum YKL-40, CHA2DS2-VASc-HSF score and cTnI
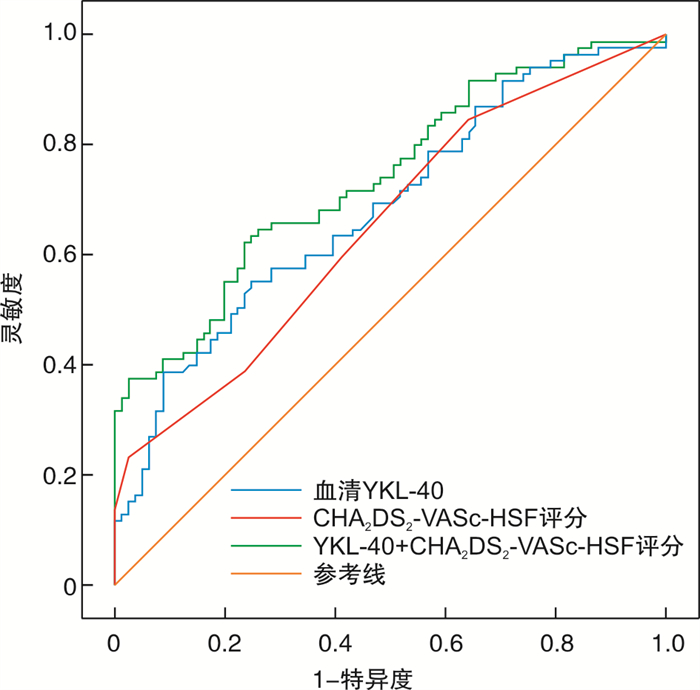
图 2 血清YKL-40、CHA2DS2-VASc-HSF评分诊断STEMI的ROC曲线
Figure 2. ROC curve of serum YKL-40, CHA2DS2-VASc-HSF score for diagnosis of STEMI
表 1 2组临床资料比较
Table 1. Comparison of clinical data between two groups
例(%), X±S, M(IQR) 项目 STEMI组(85例) 对照组(81例) t/χ2/z P 年龄/岁 60±13 62±10 6.047 0.230 男性 70(82.4) 63(77.8) 0.545 0.460 BMI/(kg·m-2) 24.26±3.57 25.32±2.92 2.22 0.029 糖尿病病史 26(30.6) 10(12.3) 8.127 0.004 高血压病史 43(50.6) 46(56.8) 0.641 0.423 既往脑卒中/TIA 31(36.5) 20(24.7) 2.704 0.100 外周血管疾病史 10(11.8) 4(4.9) 2.503 0.114 充血性心力衰竭/LVEF < 40% 11(12.9) 4(4.9) 3.232 0.072 吸烟史 56(65.9) 19(23.5) 30.141 < 0.001 冠心病家族史 16(18.8) 8(9.9) 2.685 0.101 白细胞/(×109·L-1) 10.48(4.67) 6.07(2.57) 8.464 < 0.001 血红蛋白/(g·L-1) 139.02±17.41 135.44±13.72 5.214 0.142 血小板/(×109·L-1) 211.42±59.22 200.81±55.51 0.051 0.236 甘油三酯/(mmol·L-1) 1.54(1.06) 1.43(1.11) 0.412 0.680 总胆固醇/(mmol·L-1) 4.60±1.14 4.45±1.17 0.338 0.404 LDL-C/(mmol·L-1) 2.98±0.90 2.77±0.92 0.024 0.124 HDL-C/(mmol·L-1) 1.06±0.20 1.18±0.35 14.296 0.010 血肌酐/(μmol·L-1) 73(24.70) 66.9(22.95) 1.98 0.048 尿酸/(μmol·L-1) 367.10±104.65 383.33±113.00 0.039 0.338 空腹血糖/(mmol·L-1) 6.63(3.47) 5.15(1.02) 6.027 < 0.001 LVEF/% 60.0(8.0) 62.0(6.5) 3.009 0.003 CHA2DS2-VASc-HSF评分/分 4.0(2.0) 3.0(2.0) 3.488 < 0.001 血清YKL-40/(ng·dL-1) 1072.9(1005.46) 625.2(625.69) 4.159 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 影响STEMI发生的危险因素
Table 2. Risk factors affecting the occurrence of STEMI
因素 单因素logistic回归分析 多因素logistic回归分析 β OR 95%CI P β OR 95%CI P 血清YKL-40 0.001 1.001 1.001~1.002 < 0.001 0.002 1.001 1.000~1.002 0.007 CHA2DS2-VASc-HSF评分 0.376 1.457 1.193~1.779 < 0.001 0.518 1.679 1.205~2.340 0.002 BMI -0.106 0.899 0.816~0.991 0.031 -0.078 0.925 0.791~1.081 0.326 糖尿病病史 -1.141 0.320 0.143~0.716 0.006 -0.426 0.653 0.171~2.489 0.532 吸烟史 -1.620 0.198 0.101~0.386 < 0.001 -0.811 0.445 0.163~1.211 0.113 白细胞 0.669 1.953 1.590~2.400 < 0.001 0.654 1.923 1.520~2.432 < 0.001 HDL-C -1.513 0.220 0.069~0.705 0.011 -0.257 0.773 0.107~5.566 0.773 血肌酐 0.015 1.015 1.001~1.03 0.033 0.014 1.014 0.988~1.041 0.284 空腹血糖 0.355 1.427 1.186~1.716 < 0.001 0.181 1.198 1.003~1.431 0.046 LVEF -0.049 0.952 0.911~0.995 0.030 -0.046 0.955 0.895~1.019 0.161
下载: 导出CSV
-
[1] Shen C, Ge J. Epidemic of Cardiovascular Disease in China: Current Perspective and Prospects for the Future[J]. Circulation, 2018, 138(4): 342-344. doi: 10.1161/CIRCULATIONAHA.118.033484
[2] Kastrup J. Can YKL-40 be a new inflammatory biomarker in cardiovascular disease?[J]. Immunobiology, 2012, 217(5): 483-491. doi: 10.1016/j.imbio.2011.04.007
[3] Kjaergaard AD, Johansen JS, Bojesen SE, et al. Role of inflammatory marker YKL-40 in the diagnosis, prognosis and cause of cardiovascular and liver diseases[J]. Crit Rev Clin Lab Sci, 2016, 53(6): 396-408. doi: 10.1080/10408363.2016.1190683
[4] Harutyunyan M, Gøtze JP, Winkel P, et al. Serum YKL-40 predicts long-term mortality in patients with stable coronary disease: a prognostic study within the CLARICOR trial[J]. Immunobiology, 2013, 218(7): 945-951. doi: 10.1016/j.imbio.2012.10.015
[5] Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation[J]. Chest, 2010, 137(2): 263-272. doi: 10.1378/chest.09-1584
[6] Trantalis G, Aggeli K, Toutouzas K, et al. The prognostic value of CHA2DS2-VASc and GRACE risk scores in patients with ACS[J]. Hellenic J Cardiol, 2019, 60(5): 305-308. doi: 10.1016/j.hjc.2018.03.001
[7] 李小杜, 何胜虎. CHA2DS2-VASc评分与急性ST段抬高型心肌梗死患者介入术后无复流的相关性研究[J]. 临床心血管病杂志, 2021, 37(3): 209-214. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202103005.htm
[8] Uysal OK, Turkoglu C, Duran M, et al. Predictive value of newly defined CHA2DS2-VASc-HSF score for severity of coronary artery disease in ST segment elevation myocardial infarction[J]. Kardiol Pol, 2016, 74(9): 954-960. doi: 10.5603/KP.a2016.0054
[9] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 47(10): 766-783. https://www.cnki.com.cn/Article/CJFDTOTAL-GWXX201504001.htm
[10] Montecucco F, Carbone F, Schindler TH. Pathophysiology of ST-segment elevation myocardial infarction: novel mechanisms and treatments[J]. Eur Heart J, 2016, 37(16): 1268-1283. doi: 10.1093/eurheartj/ehv592
[11] Liuzzo G, Biasucci LM, Gallimore JR, et al. The prognostic value of C-reactive protein and serum amyloid a protein in severe unstable angina[J]. N Engl J Med, 1994, 331(7): 417-424. doi: 10.1056/NEJM199408183310701
[12] Toss H, Lindahl B, Siegbahn A, et al. Prognostic influence of increased fibrinogen and C-reactive protein levels in unstable coronary artery disease. FRISC Study Group. Fragmin during Instability in Coronary Artery Disease[J]. Circulation, 1997, 96(12): 4204-4210. doi: 10.1161/01.CIR.96.12.4204
[13] 鲍微, 徐燕. 血清总胆红素、C反应蛋白及脂蛋白a与高脂血症患者的关系研究[J]. 临床血液学杂志, 2020, 33(6): 422-424. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202006012.htm
[14] Tong X, Wang D, Liu S, et al. The YKL-40 protein is a potential biomarker for COPD: a meta-analysis and systematic review[J]. Int J Chron Obstruct Pulmon Dis, 2018, 13: 409-418. doi: 10.2147/COPD.S152655
[15] Johansen JS, Schultz NA, Jensen BV. Plasma YKL-40: a potential new cancer biomarker?[J]. Future Oncol, 2009, 5(7): 1065-1082. doi: 10.2217/fon.09.66
[16] Rehli M, Niller HH, Ammon C, et al. Transcriptional regulation of CHI3 L1, a marker gene for late stages of macrophage differentiation[J]. J Biol Chem, 2003, 278(45): 44058-44067. doi: 10.1074/jbc.M306792200
[17] Baeten D, Boots AM, Steenbakkers PG, et al. Human cartilage gp-39+, CD16+ monocytes in peripheral blood and synovium: correlation with joint destruction in rheumatoid arthritis[J]. Arthritis Rheum, 2000, 43(6): 1233-1243. doi: 10.1002/1529-0131(200006)43:6<1233::AID-ANR6>3.0.CO;2-9
[18] Zheng JL, Lu L, Hu J, et al. Increased serum YKL-40 and C-reactive protein levels are associated with angiographic lesion progression in patients with coronary artery disease[J]. Atherosclerosis, 2010, 210(2): 590-595. doi: 10.1016/j.atherosclerosis.2009.12.016
[19] 倪占玲, 杨宏辉, 陈岩, 等. 血清YKL-40水平与冠状动脉罪犯血管斑块易损性的相关性研究[J]. 临床心血管病杂志, 2019, 35(5): 402-406. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB201905004.htm
[20] Wang Y, Ripa RS, Johansen JS, et al. YKL-40 a new biomarker in patients with acute coronary syndrome or stable coronary artery disease[J]. Scand Cardiovasc J, 2008, 42(5): 295-302. doi: 10.1080/14017430802220567
[21] Uysal OK, Duran M, Ozkan B, et al. Red cell distribution width is associated with acute myocardial infarction in young patients[J]. Cardiol J, 2012, 19(6): 597-602. doi: 10.5603/CJ.2012.0111
[22] Kaya MG, Uyarel H, Akpek M, et al. Prognostic value of uric acid in patients with ST-elevated myocardial infarction undergoing primary coronary intervention[J]. Am J Cardiol, 2012, 109(4): 486-491. doi: 10.1016/j.amjcard.2011.09.042
[23] Nacar AB, Erayman A, Kurt M, et al. The relationship between coronary collateral circulation and neutrophil/lymphocyte ratio in patients with coronary chronic total occlusion[J]. Med Princ Pract, 2015, 24(1): 65-69. doi: 10.1159/000365734
[24] 张妮, 向定成, 张金霞, 等. 吸烟对不同性别、年龄人群急性ST段抬高型心肌梗死发病风险的相关性研究[J]. 中国循环杂志, 2016, 31(9): 858-861. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH201609007.htm
[25] 王宇, 彭晓恩, 薛铮, 等. 联合检测IMA、cTnI、CK-MB早期诊断急性冠脉综合征的应用价值[J]. 中西医结合心脑血管病杂志, 2018, 16(2): 211-212. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYY201802024.htm
[26] 郭瑞敏, 邵周俊, 孙燕妮, 等. 在急诊胸痛患者中急性炎症指数与入院即刻hs-cTNI相关分析[J]. 临床急诊杂志, 2019, 20(1): 45-51. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC201901010.htm
[27] 朱秀菊, 王艳华, 沈芳. 高敏cTnI在急性心肌梗死患者中的诊断阈值与影响因素分析[J]. 国际检验医学杂志, 2016, 37(18): 2545-2547. https://www.cnki.com.cn/Article/CJFDTOTAL-GWSQ201618015.htm
[28] 曾光豪, 卢攀, 金杰. 入院3 h内超敏肌钙蛋白I绝对变化值及其变化斜率对急性心肌梗死的预测价值[J]. 临床急诊杂志, 2020, 21(11): 909-912. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202011013.htm
-
图(2)
表(2)
计量
- 文章访问数: 1063
- PDF下载数: 352
- 施引文献: 0