
A new model for predicting major adverse cardiovascular events after PCI surgery: based on Super Learner algorithm
-
摘要: 目的 建立多种基于集成学习的经皮冠状动脉介入(PCI)预测模型,从而筛选出最佳的预测模型组合及变量。方法 本研究纳入2018年1月—2022年6月所有符合PCI手术标准并行PCI术的心肌梗死患者,采用Cox回归对变量进行筛选,根据不同的单一模型组合通过五折交叉验证建立Super Learner(SL)模型,并用ROC曲线和PR曲线对各个模型进行评价。结果 本次研究共收集到3 880例PCI患者,平均年龄为64.46岁,其中大部分是男性(73.8%)和高血压(57.2%)。Cox回归共筛选出24个相关变量,最终共建立4个SL模型,预测能力在测试集上表现均较好,AUC值均在0.84以上,而PRC值均在0.72以上,其中混合模型1表现最佳(AUC:0.846,PRC:0.729)。预测变量中住院次数、是否肾功能不全、病变冠脉支数等是各个混合模型中的重要变量,且与主要不良心血管事件(MACE)发生呈正相关。结论 这项研究为PCI预后影响因素研究及SL模型在PCI领域的应用增加了证据。住院次数、肾功能不全、病变冠脉支数、Cre等对MACE的发生有一定影响,术前有效改善其肾功能降低MACE的发生。而Super Learner模型作为集成学习的实际应用之一,有效提高了整体预测模型的稳定性及适用性,同时证明了在PCI术预后上的应用价值。
-
关键词:
- 集成学习 /
- Super Learner /
- 经皮冠状动脉介入术 /
- 主要不良心血管事件
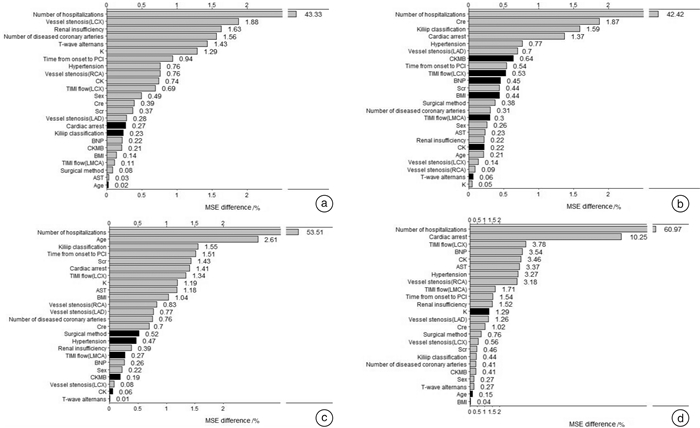
Abstract: Objective To establish a variety of PCI prediction models based on ensemble learning to screen the best combination of prediction models and variables.Methods In this study, all patients who met the criteria for PCI and underwent PCI from January 2018 to June 2022 were included. The variables were screened by Cox regression, and the Super Learner model was established by 5-fold cross-validation according to different single model combinations. ROC curve and PR curve were used to evaluate each model.Results A total of 3880 patients with PCI were included in the study, with the average age of 64.46 years old. Most of them were male(73.8%) and had hypertension(57.2%). Twenty-four related variables were screened out by Cox regression and four SL models were finally established. The prediction abilities of the four SL models were all good on the test set, with the AUC values above 0.84 and the PRC values above 0.72, among which the hybrid model 1 performed the best(AUC: 0.846 and PRC: 0.729). The number of hospitalizations, renal insufficiency or not, and the number of diseased coronary artery branches were important variables in each mixed model among the prediction variables, and they were positively correlated with the occurrence of MACE.Conclusion This study provides additional evidence for that study of prognostic factors of PCI and the application of SL model in PCI. The times of hospitalization, renal insufficiency, the number of diseased coronary artery branches, and Cre have a certain influence on the occurrence of MACE. Effective improvement of renal function before surgery can reduce the occurrence of MACE. As one of the practical applications of ensemble learning, Super Learner model effectively improves the stability and applicability of the overall prediction model, and proves its application value in the prognosis of PCI.-
Key words:
- ensemble learning /
- Super Learner /
- PCI /
- MACE
-

-
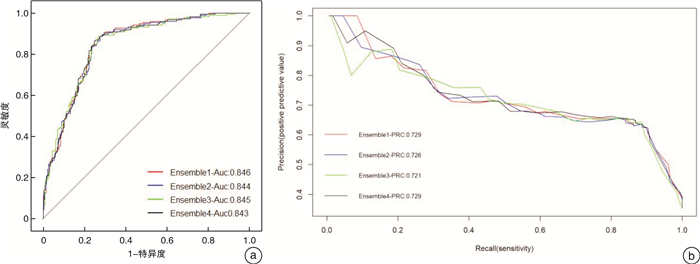
图 2 各集成模型在测试集中的ROC图和PR图
Figure 2. ROC diagram and PR diagram of each integration model in the test set
表 1 患者基本特征
Table 1. General data
例(%), M(P25, P75) 项目 总人数(3 880例) MACE组(706例) 非MACE组(3 174例) 年龄/岁 65(57,72) 65(58,73) 65(57,72) 男性 2 862(73.8) 543(76.9) 2 319(73.1) 既往病史 高血压 2 220(57.2) 423(59.9) 1 797(56.6) 高脂血症 1 117(28.8) 192(27.2) 925(29.1) 糖尿病 1 151(29.7) 235(33.3) 916(28.9) 肾功能不全 523(13.5) 105(14.9) 418(13.2) 肺部感染 353(9.1) 69(9.8) 284(8.9) 吸烟史 1 324(34.1) 247(35.0) 1 077(33.9) 饮酒史 933(24.0) 172(24.4) 761(24.0) 家族史 糖尿病 83(2.1) 21(3.0) 62(2.0) 高血压 161(4.1) 30(4.2) 131(4.1) 冠心病 71(1.8) 16(2.3) 55(1.7) 心电图 窦性心律 3 701(95.4) 673(95.3) 3 028(95.4) 心房颤动 172(4.4) 30(4.2) 142(4.5) 起搏心律 374(9.6) 67(9.5) 307(9.7) 三度及高度房室传导阻滞 76(2.0) 15(2.1) 61(1.9) ST段改变 1 623(41.8) 296(41.9) 1 327(41.8) 完全性左束支传导阻滞 60(1.5) 13(1.8) 47(1.5) 完全性右束支传导阻滞 225(5.8) 43(6.1) 182(5.7) 异常Q波 1 058(27.3) 201(28.5) 857(27.0) 左心室高电压 545(14.0) 100(14.2) 445(14.0) T波倒置 1 131(29.1) 221(31.3) 910(28.7) Kiliip分级 Ⅰ 249(6.4) 43(6.1) 206(6.5) Ⅱ 1 772(45.7) 309(43.8) 1 463(46.1) Ⅲ 1 508(38.9) 303(42.9) 1 205(38.0) Ⅳ 154(4.0) 28(4.0) 126(4.0) 住院次数 1次 2 319(59.8) 65(9.2) 2 254(71.0) 2次 857(22.1) 344(48.7) 513(16.2) 3次 434(11.2) 222(31.4) 212(6.7) 4次 92(2.4) 36(5.1) 56(1.8) 病变冠脉支数 1支 923(23.8) 111(15.7) 812(25.6) 2支 1 175(30.3) 181(25.6) 994(31.3) 3支 1 568(40.4) 354(50..1) 1 214(38.2) 4支 214(5.5) 60(8.5) 154(4.9) BMI/(kg/m2) 23.9(22.0,25.7) 23.9(22.0,25.7) 23.9(22.0,25.7) 脉搏/(次/min) 87(80,94) 88(80,94) 87(80,94) 收缩压/mmHg 129(115,145) 129(115,145) 129(115,145) 舒张压/mmHg 70(63,77) 70(63,76) 70(63,78) 血液检查 BNP/(pg/mL) 150.3(50.0,445.7) 186.4(62.7,527.5) 144.5(48.4,424.3) AST/(U/L) 28.3(21.2,54.1) 27.9(20.8,50.5) 28.3(21.2,54.8) CK/(U/L) 126.5(82.0,317.9) 124.3(78.2,325.1) 126.9(82.9,317.0) CKMB/(U/L) 19.8(13.7,39.9) 18.9(13.2,39.1) 19.9(13.9,40.0) Cre/(mmol/L) 81.8(68.6,99.7) 84.5(71.8,104.6) 81.1(67.8,98.6) eGFR/[mL·min-1·(1.73m2)-1] 82.4(65.1,99.0) 78.9(61.1,95.9) 83.1(65.8,99.8) Scr/(mL/min) 66.9(48.0,87.5) 64.5(46.8,83.3) 67.4(48.2,87.9) K/(mmol/L) 3.9(3.6,4.2) 3.9(3.6,4.2) 3.9(3.6,4.2) PCI手术信息 心脏骤停 58(1.5) 16(2.3) 42(1.3) 从发病到PCI的时间 < 3 h 189(4.9) 39(5.5) 150(4.7) 3~6 h 202(5.2) 42(5.9) 160(5.0) 6~9 h 362(9.3) 75(10.6) 287(9.0) 9~12 h 359(9.3) 65(9.2) 294(9.3) >12 h 2 630(67.8) 453(64.2) 2 177(68.6) 介入途径 股动脉 178(4.6) 39(5.5) 139(4.4) 桡动脉 3 676(94.7) 662(93.8) 3 014(95.0) 尺动脉 26(0.7) 5(0.7) 21(0.7) 手术方式 血栓抽吸 44(1.1) 9(1.3) 35(1.1) PTCA 3 595(92.7) 657(93.1) 2 938(92.6) 支架植入 241(6.2) 40(5.7) 201(6.3)  下载: 导出CSV
下载: 导出CSV
表 2 各集成模型的组成
集成模型 Em1 Em2 Em3 Em4 randomForest × × √ × cforest √ √ √ × glm × × √ × step √ × √ × glmnet √ × √ × xgboost × × √ √ ipredbagg × × √ √ gbm √ √ √ √ nnls × × √ √ svm √ × √ × lm × × √ ×
下载: 导出CSV
-
[1] 国家心血管病中心. 中国心血管健康与疾病报告2021[M]. 北京: 科学出版社, 2022: 100.
[2] Al-Lamee RK, Nowbar AN, Francis DP. Percutaneous coronary intervention for stable coronary artery disease[J]. Heart, 2019, 105(1): 11-19. doi: 10.1136/heartjnl-2017-312755
[3] Teoh Z, Al-Lamee RK. Courage O. Percutaneous Coronary Intervention for Stable Coronary Artery Disease[J]. Interv Cardiol Clin, 2020, 9(4): 469-482.
[4] Groenland FTW, Neleman T, Kakar H, et al. Intravascular ultrasound-guided versus coronary angiography-guided percutaneous coronary intervention in patients with acute myocardial infarction: A systematic review and meta-analysis[J]. Int J Cardiol, 2022, 353: 35-42. doi: 10.1016/j.ijcard.2022.01.021
[5] Abtan J, Wiviott SD, Sorbets E, et al. Prevalence, clinical determinants and prognostic implications of coronary procedural complications of percutaneous coronary intervention in non-ST-segment elevation myocardial infarction: Insights from the contemporary multinational TAO trial[J]. Arch Cardiovasc Dis, 2021, 114(3): 187-196. doi: 10.1016/j.acvd.2020.09.005
[6] 刘健迪, 龚韧, 夏华松, 等. 高密度脂蛋白胆固醇水平对药物洗脱支架植入后早期血管愈合的影响[J]. 临床心血管病杂志, 2022, 38(2): 123-131. doi: 10.13201/j.issn.1001-1439.2022.02.009 https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.02.009
[7] 徐慧慧, 谢艳辉, 宋恒良, 等. PCSK9抑制剂对急性ST段抬高型心肌梗死PCI术后的微循环功能及左心室重构的影响[J]. 临床心血管病杂志, 2022, 38(1): 22-28. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.01.005
[8] Xu B, Tu S, Song L, et al. Angiographic quantitative flow ratio-guided coronary intervention(FAVOR Ⅲ China): a multicentre, randomised, sham-controlled trial[J]. Lancet, 2021, 398(10317): 2149-2159. doi: 10.1016/S0140-6736(21)02248-0
[9] Madhavan MV, Kirtane AJ, Redfors B, et al. Stent-related adverse events>1 year after percutaneous coronary intervention[J]. J Am Coll Cardiol, 2020, 75(6): 590-604. doi: 10.1016/j.jacc.2019.11.058
[10] Chen Z, Duan J, Kang L, et al. Class-imbalanced deep learning via a class-balanced ensemble[J]. IEEE Trans Neural Netw Learn Syst, 2021, 22: 100.
[11] El Asnaoui K. Design ensemble deep learning model for pneumonia disease classification[J]. Int J Multimed Inf Retr, 2021, 10(1): 55-68. doi: 10.1007/s13735-021-00204-7
[12] Chen Z, Li Q, Li R, et al. Ensemble learning accurately predicts the potential benefits of thrombolytic therapy in acute ischemic stroke[J]. Quant Imaging Med Surg, 2021, 11(9): 3978-3989. doi: 10.21037/qims-21-33
[13] van der Laan MJ, Polley EC, et al. Super learner[J]. Stat Appl Genet Mol Biol, 2007, 6: 25.
[14] Wardenaar KJ, Riese H, Giltay EJ, et al. Common and specific determinants of 9-year depression and anxiety course-trajectories: A machine-learning investigation in the Netherlands Study of Depression and Anxiety(NESDA)[J]. J Affect Disord, 2021, 293: 295-304. doi: 10.1016/j.jad.2021.06.029
[15] Cartus AR, Naimi AI, Himes KP, et al. Can ensemble machine learning improve the accuracy of severe maternal morbidity screening in a perinatal database?[J]. Epidemiology, 2022, 33(1): 95-104. doi: 10.1097/EDE.0000000000001433
[16] Murnane PM, Ayieko J, Vittinghoff E, et al. Machine learning algorithms using routinely collected data do not adequately predict viremia to inform targeted services in postpartum women living with HIV[J]. J Acquir Immune Defic Syndr, 2021, 88(5): 439-447. doi: 10.1097/QAI.0000000000002800
[17] 徐芳, 徐俊杰, 吴春苑, 等. 左室心肌做功对急性心肌梗死患者急诊PCI术后MACE发生的预测价值[J]. 临床心血管病杂志, 2022, 38(12): 960-966. doi: 10.13201/j.issn.1001-1439.2022.12.007 https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.12.007
[18] Yiannoullou P, Summers A, Goh SC, et al. Major adverse cardiovascular events following simultaneous pancreas and kidney transplantation in the united kingdom[J]. Diabetes Care, 2019, 42(4): 665-673. doi: 10.2337/dc18-2111
[19] Polley E, LeDell E, Kennedy C, van der Laan M. SuperLearner: SuperLearner Prediction[J]. Rpackage Version, 20210, 20: 100.
[20] Stef van B, Karin GO. Multivariate imputation by chained equations in R[J]. J Statist Software, 2011, 45(3), 1-67.
[21] Kuhn M. Classification and regression training[J]. Rpackage Version, 2022, 20: 100.
[22] He H, Garcia EA. Learning from imbalanced data[J]. IEEE Trans Knowl Data Eng, 2009, 21(9): 1263-1284. doi: 10.1109/TKDE.2008.239
[23] Blum M, Cao D, Chandiramani R, et al. Prevalence and prognostic impact of hsCRP elevation are age-dependent in women but not in men undergoing percutaneous coronary intervention[J]. Catheter Cardiovasc Interv, 2021, 97(7): E936-E944.
[24] Liu S, Yang S, Xing A, et al. Machine learning-based long-term outcome prediction in patients undergoing percutaneous coronary intervention[J]. Cardiovasc Diagn Ther, 2021, 11(3): 736-743. doi: 10.21037/cdt-21-37
[25] Kulkarni H, Thangam M, Amin AP. Artificial neural network-based prediction of prolonged length of stay and need for post-acute care in acute coronary syndrome patients undergoing percutaneous coronary intervention[J]. Eur J Clin Invest, 2021, 51(3): e13406.
[26] Druchok M, Yarish D, Garkot S, et al. Ensembling machine learning models to boost molecular affinity prediction[J]. Comput Biol Chem, 2021, 93: 107529. doi: 10.1016/j.compbiolchem.2021.107529
[27] El Asnaoui K. Design ensemble deep learning model for pneumonia disease classification[J]. Int J Multimed Inf Retr, 2021, 10(1): 55-68. doi: 10.1007/s13735-021-00204-7
[28] Naimi AI, Balzer LB. Stacked generalization: an introduction to super learning[J]. Eur J Epidemiol, 2018, 33(5): 459-464. doi: 10.1007/s10654-018-0390-z
[29] Golmakani MK, Polley EC. Super learner for survival data prediction[J]. Int J Biostat, 2020, 20: 100.
[30] Ehwerhemuepha L, Danioko S, Verma S, et al. A super learner ensemble of 14 statistical learning models for predicting COVID-19 severity among patients with cardiovascular conditions[J]. Intell Based Med, 2021, 5: 100030.
[31] Biswas S, Dinh D, Lucas M, et al. Incidence and predictors of unplanned hospital readmission after percutaneous coronary intervention[J]. J Clin Med, 2020, 9(10): 3242.
[32] Harjai KJ, Thompson HW, Turgut T, et al. Simple clinical variables are markers of the propensity for readmission in patients hospitalized with heart failure[J]. Am J Cardiol, 2001, 87(2): 234-239.
[33] Hummel SL, Katrapati P, Gillespie BW, et al. Impact of prior admissions on 30-day readmissions in medicare heart failure inpatients[J]. Mayo Clin Proc, 2014, 89(5): 623-630.
[34] Kilkenny MF, Dewey HM, Sundararajan V, et al. Readmissions after stroke: linked data from the Australian Stroke Clinical Registry and hospital databases[J]. Med J Aust, 2015, 203(2): 102-106.
[35] Dibben G, Faulkner J, Oldridge N, et al. Exercise-based cardiac rehabilitation for coronary heart disease[J]. Cochrane Database Syst Rev, 2021, 11(11): CD001800.
[36] Qi L, Liu H, Cheng L, et al. Impact of renal insufficiency on prognosis of patients with acute coronary syndrome[J]. Int J Gen Med, 2021, 14: 8919-8927.
[37] Chiang CY, Huang SC, Chen M, et al. Effects of renal impairment on cardiac remodeling and clinical outcomes after myocardial infarction[J]. Int J Med Sci, 2021, 18(13): 2842-2848.
[38] Deguchi Y, Saito Y, Nakao M, et al. Trajectory of renal function change and kidney injury after percutaneous coronary intervention in patients with stable coronary artery disease[J]. Heart Vessels, 2021, 36(3): 315-320.
[39] Khoury S, Margolis G, Ravid D, et al. Outcomes of early and reversible renal impairment in patients with ST segment elevation myocardial infarction undergoing percutaneous coronary intervention[J]. Eur Heart J Acute Cardiovasc Care, 2020, 9(7): 684-689.
[40] Sciahbasi A, Cuono A, Marrangoni A, et al. Acute kidney injury and multivessel percutaneous coronary interventions in chronic renal disease: the AMICI study[J]. Minerva Cardiol Angiol, 2021, 69(5): 491-498.
[41] Ammirati AL. Chronic kidney disease[J]. Rev Assoc Med Bras, 2020, 66: s03-s09.
[42] Schefold JC, Filippatos G, Hasenfuss G, et al. Heart failure and kidney dysfunction: epidemiology, mechanisms and management[J]. Nat Rev Nephrol, 2016, 12(10): 610-623.
-

图(3)
表(2)
计量
- 文章访问数: 1386
- PDF下载数: 297
- 施引文献: 0