
Interpretation of the 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
-
摘要: 2023 ESC急性和慢性心力衰竭诊断和治疗指南更新要点是在2021 ESC心力衰竭指南基础上,借助16项高质量循证医学证据,对慢性心力衰竭、急性心力衰竭、心力衰竭合并症和预防三大方面的诊疗建议作出更新。钠-葡萄糖共转运蛋白2抑制剂(sodium-glucose cotransporter 2 inhibitor,SGLT2i)改变了心力衰竭治疗格局,成为首个慢性心力衰竭全射血分数谱应用的药物。急性心力衰竭稳定期建议及早使用SGTL2i,尽早启动指南指导的药物并快速滴定。SGLT2i和新型醛固酮受体拮抗剂非奈利酮被推荐用于慢性肾病合并2型糖尿病患者以预防心力衰竭。Abstract: Based on 16 high-quality randomized clinical trials and related meta-analysis, the 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure was released and provided updated recommendations for the following sections of the 2021 ESC heart failure(HF) guidelines: chronic HF including HF with mildly reduced ejection fraction(HFmrEF) and preserved ejection fraction(HFpEF), acute HF and comorbidities and prevention of HF. Sodium glucose cotransporter 2 inhibitor(SGLT2i) has changed the treatment pattern of chronic heart failure, and it is the first drug to be recommended across the ejection fraction spectrum. During the stable phase of acute HF, it is recommended to use SGTL2i as soon as possible and to start the guideline-directed medical therapy as soon as possible, and perform rapid titration. SGLT2i and a new aldosterone receptor antagonist, Finerenone, have been recommended for the prevention of heart failure in patients with chronic kidney disease and type 2 diabetes mellitus.
-

-
表 1 HFrEF、HFmrEF和HFpEF的定义
Table 1. Definition of heart failure
心衰类型 HFrEF HFmrEF HFpEF 1 症状±体征a) 症状±体征a) 症状±体征a) 标准 2 LVEF ≤40% LVEF 41%~49%b) LVEF ≥50% 3 - - 有客观证据表明心脏结构和(或)功能异常与左室舒张功能障碍/左室充盈压升高一致,包括钠尿肽升高c) 注:HFrEF:射血分数降低心衰;HFmrEF:射血分数轻度降低心衰;HFpEF:射血分数保留心衰;LVEF:左心室射血分数。a)在心衰的早期阶段(特别是HFpEF)和经过最佳治疗的患者中,可能不存在体征;b)对于HFmrEF的诊断,存在其他心脏结构异常的证据(如左房增大、左室肥厚或超声心动图测量左室充盈受损)使诊断更有可能;c)对于HFpEF的诊断,存在的客观证据越多,HFpEF的可能性越高。  下载: 导出CSV
下载: 导出CSV
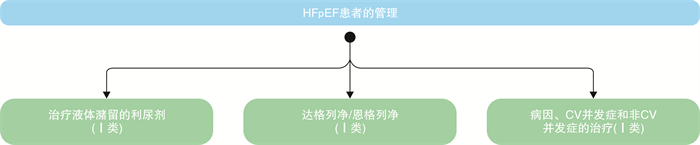
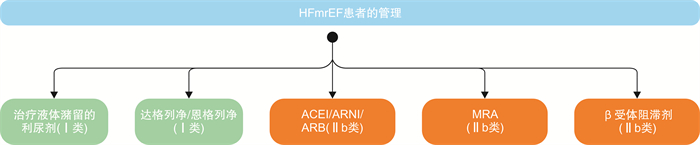
表 2 对HFmrEF和HFpEF患者的治疗建议
Table 2. Treatment recommendations for patients with HF
推荐 推荐等级 证据水平 HFmrEF患者予以SGLT2i(达格列净或恩格列净),以降低心衰住院或心血管死亡风险 Ⅰ A HFpEF患者予以SGLT2i(达格列净或恩格列净),以降低心衰住院或心血管死亡风险 Ⅰ A
下载: 导出CSV
表 3 对急性心衰住院患者出院前和出院后早期随访的建议
Table 3. Recommendations before and after discharge
推荐 推荐等级 证据水平 在急性心衰患者出院前及出院后6周内的随访中,予以强化的管理策略,早期启动并快速滴定有循证依据的药物,以降低心衰再住院或死亡的风险 Ⅰ B
下载: 导出CSV
表 4 慢性肾病合并2型糖尿病患者心衰预防的建议
Table 4. Recommendations for prevention of HF in patients with chronic kidney disease and type 2 diabetes mellitus
推荐 推荐等级 证据水平 慢性肾病合并2型糖尿病患者予以SGLT2i,以降低心衰住院或心血管死亡的风险 I A 慢性肾病合并2型糖尿病患者予以非奈利酮,以降低心衰住院的风险 I A
下载: 导出CSV
表 5 心衰合并铁缺乏的建议
Table 5. Recommendations for heart failure with iron deficiency
推荐 推荐等级 证据水平 症状性HFrEF和HFmrEF合并铁缺乏患者予以静脉补充铁剂,以缓解心衰症状并提高生活质量 Ⅰ A 症状性HFrEF和HFmrEF合并铁缺乏患者,应考虑予以静脉补充羧基麦芽糖酐铁或去异麦芽糖酐铁,以降低心衰住院风险 Ⅱa B
下载: 导出CSV
-
[1] McDonagh TA, Metra M, Adamo M, et al. ESC Scientific Document Group. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J, 2023, Aug 25, doi: 10.1093/eurheartj/ehad195.
[2] Kosiborod MN, Angermann CE, Collins SP, et al. Effects of Empagliflozin on Symptoms, Physical Limitations, and Quality of Life in Patients Hospitalized for Acute Heart Failure: Results From the EMPULSE Trial[J]. Circulation, 2022, 146(4): 279-288. doi: 10.1161/CIRCULATIONAHA.122.059725
[3] Mentz RJ, Garg J, Rockhold FW, et al. Ferric Carboxymaltose in Heart Failure with Iron Deficiency[J]. N Engl J Med, 2023, 389(11): 975-986. doi: 10.1056/NEJMoa2304968
[4] 廖梦阳, 廖玉华, 余淼, 等. SGLT2抑制剂治疗心力衰竭潜在机制的新认识[J]. 临床心血管病杂志, 2022, 38(1): 1-6. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.01.001
-
图(2)
表(5)
计量
- 文章访问数: 1513
- PDF下载数: 1775
- 施引文献: 0