
A meta-analysis of the evaluation of early invasive and early conservative treatment effects in patients over 75 years of age with non-ST-elevation acute coronary syndrome
-
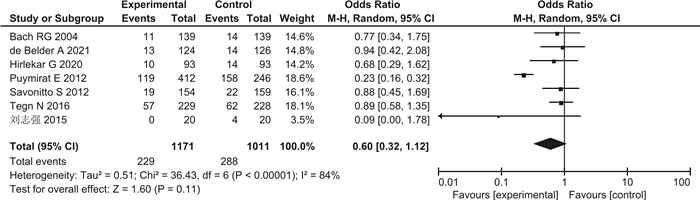
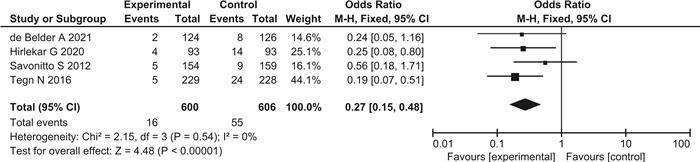
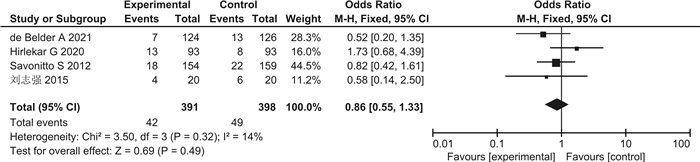
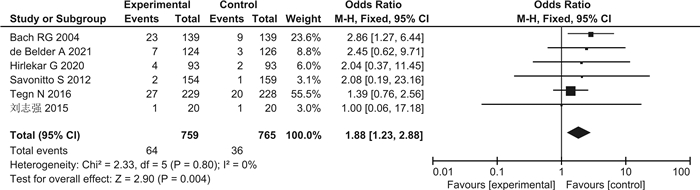
摘要: 目的 评价75岁以上老年非ST段抬高型急性冠状动脉综合征(NSTE-ACS)患者早期侵入性与早期保守治疗效果。方法 检索Embase、Medline、Cochrane Library、PubMed、VIP、万方、CNKI等数据库,检索自建库至2023年4月12日的所有随机对照研究。结果 共纳入7篇研究。保守组与侵入组非致死性心肌梗死(OR=0.50,95%CI 0.37~0.67,P<0.00001)、血运重建(OR=0.27,95%CI 0.15~0.48,P<0.00001)及出血发生率(OR=1.88,95%CI 1.23~2.88,P=0.004)差异有统计学意义,全因死亡或非致死性心肌梗死复合终点(OR=0.78,95%CI 0.55~1.11,P=0.16)、全因死亡(OR=0.60,95%CI 0.32~1.12,P=0.11)、心血管死亡(OR=0.97,95%CI 0.47~1.99,P=0.93)、再入院率(OR=0.86,95%CI 0.55~1.33,P=0.49)差异无统计学意义。结论 在75岁以上的NSTE-ACS患者中,与保守组相比,侵入组显著降低了非致死性心肌梗死和血运重建的发生率,但显著增加了出血的风险。
-
关键词:
- 非ST段抬高型急性冠状动脉综合征 /
- 早期侵入治疗 /
- 药物保守治疗 /
- meta分析
Abstract: Objective To assess the effects of early invasive versus early conservative treatment in elderly patients over 75 years of age with non-ST-elevation acute coronary syndrome(NSTE-ACS).Methods Embase, Medline, Cochrane Library, PubMed, VIP, Wanfang, CNKI and other databases were searched, and all randomized controlled studies were searched from the establishment of the library to April 12, 2023.Results A total of seven studies were included. There were significant differences in non-fatal myocardial infarction[OR=0.50, 95%CI(0.37, 0.67), P < 0.00001], revascularization[OR=0.27, 95%CI(0.15, 0.48), P < 0.00001]and bleeding incidence[OR=1.88, 95%CI(1.23, 2.88), P=0.004]between the invasion group and conservative group. In the composite endpoint of all-cause death or nonfatal myocardial infarction[OR=0.78, 95%CI(0.55, 1.11), P=0.16], all-cause mortality[OR=0.60, 95%CI(0.32, 1.12), P=0.11], cardiovascular death[OR=0.97, 95%CI(0.47, 1.99), P=0.93], readmission rate[OR=0.86, 95%CI(0.55, 1.33), P=0.49], the differences were not statistically significant.Conclusion In patients older than 75 years of NSTE-ACS, the incidence of nonfatal myocardial infarction and revascularization were significantly reduced in the invasive group, but the risk of bleeding significantly increased in the conservative group. -

-
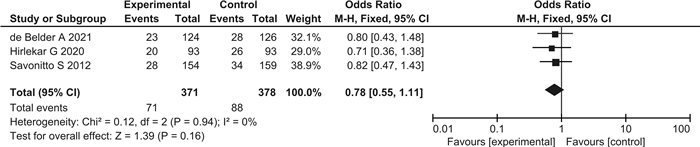
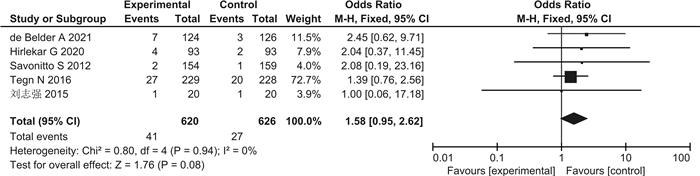
图 3 全因死亡或非致死性心肌梗死复合终点森林图
Figure 3. Forest map of composite endpoint of all-cause or non-fatal myocardial infarction
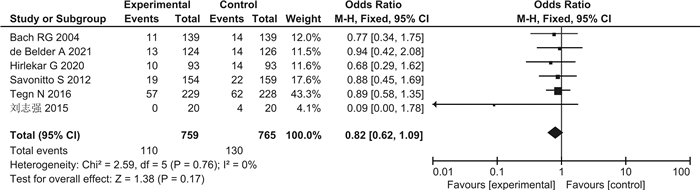
图 5 全因死亡率森林图(剔除Puymirat等的研究)
Figure 5. Forest map of all-cause mortality(excluding Puymirat et al.)
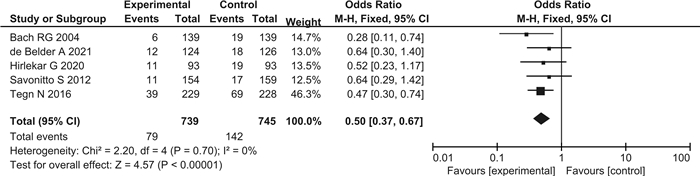
图 6 非致死性心肌梗死发生率森林图
Figure 6. Forest map of incidence of nonfatal myocardial infarction
表 1 纳入文献的基本特征
Table 1. General data
第1作者/年份 例数 男/女/例 年龄/岁 研究对象 疗程 结局指标 侵入组 保守组 de Belder A 2021[7] 124 126 112/138 ≥80 NSTEMI 1年 ①②③⑤⑥⑦ Hirlekar G 2020[8] 93 93 102/84 ≥80 NSTEACS 1年 ①②③⑤⑥⑦ Tegn N 2016[9] 229 228 225/232 ≥80 NSTEACS 1.53年 ②③⑤⑦ Savonitto S 2012[10] 154 159 157/156 >75 NSTEACS 1年 ①②③④⑤⑥⑦ Puymirat E 2012[11] 412 246 - 提取>75岁患者 NSTEMI 3年 ② Bach RG 2004[12] 139 139 - 提取>75岁患者 NSTEACS 6个月 ②③⑦ 刘志强2015[13] 20 20 - >75 NSTEMI 1年 ②⑥⑦ 注:①全因死亡或非致死性心肌梗死复合终点;②全因死亡率;③非致死性心肌梗死发生率;④心血管死亡发生率;⑤血运重建发生率;⑥再入院率;⑦出血发生率。  下载: 导出CSV
下载: 导出CSV
-
[1] Severino P, D'Amato A, Prosperi S, et al. Myocardial Infarction with Non-Obstructive Coronary Arteries(MINOCA): focus on coronary microvascular dysfunction and genetic susceptibility[J]. J Clin Med, 2023, 12(10): 3586. doi: 10.3390/jcm12103586
[2] 黄成茜, 梁鹏, 郭福佳, 等. H型高血压患者并发脑梗死与血清MCP-1、MCPIP1的相关性分析[J]. 临床心血管病杂志, 2022, 38(10): 786-790. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.10.006
[3] Hoo JX, Yang YF, Tan JY, et al. Impact of multicomponent integrated care on mortality and hospitalization after acute coronary syndrome: a systematic review and meta-analysis[J]. Eur Heart J Qual Care Clin Outcomes, 2023, 9(3): 258-267. doi: 10.1093/ehjqcco/qcac032
[4] Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review[J]. JAMA, 2022, 327(7): 662-675. doi: 10.1001/jama.2022.0358
[5] Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation[J]. Rev Esp Cardiol(Engl Ed), 2021, 74(6): 544.
[6] Mantovani F, Campo G, Guerri E, et al. Management and outcomes in the elderly with non-ST-elevation acute coronary syndromes admitted to spoke hospitals with no catheterization laboratory facility[J]. J Clin Med, 2022, 11(20): 6179. doi: 10.3390/jcm11206179
[7] de Belder A, Myat A, Blaxill J, et al. Revascularisation or medical therapy in elderlypatients with acute anginal syndromes: the RINCAL randomised trial[J]. Euro Intervention, 2021, 17(1): 67-74.
[8] Hirlekar G, Libungan B, Karlsson T, et al. Percutaneous coronary intervention in the very elderly with NSTE-ACS: the randomized 80+ study[J]. Scand Cardiovasc J, 2020, 54(5): 315-321. doi: 10.1080/14017431.2020.1781243
[9] Tegn N, Abdelnoor M, Aaberge L, et al. Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris(After Eighty study): an open-label randomised controlled trial[J]. Lancet, 2016, 387(10023): 1057-1065. doi: 10.1016/S0140-6736(15)01166-6
[10] Savonitto S, Cavallini C, Petronio AS, et al. Italian Elderly ACS Trial Investigators. Early aggressive versus initially conservative treatment in elderly patients with non-ST-segment elevation acute coronary syndrome: a randomized controlled trial[J]. JACC Cardiovasc Interv, 2012, 5(9): 906-916. doi: 10.1016/j.jcin.2012.06.008
[11] Puymirat E, Taldir G, Aissaoui N, et al. Use of invasive strategy in non-ST-segment elevation myocardial infarction is a major determinant of improved long-term survival: FAST-MI(French Registry of Acute Coronary Syndrome)[J]. JACC Cardiovasc Interv, 2012, 5(9): 893-902. doi: 10.1016/j.jcin.2012.05.008
[12] Bach RG, Cannon CP, Weintraub WS, et al. The effect of routine, early invasive management on outcome for elderly patients with non-ST-segment elevation acute coronary syndromes[J]. Ann Intern Med, 2004, 141(3): 186-195. doi: 10.7326/0003-4819-141-3-200408030-00007
[13] 刘志强, 赵利培, 李医博, 等. 高龄高危女性急性非ST段抬高型心肌梗死早期侵入治疗与保守治疗的效果分析[J]. 中国煤炭工业医学杂志, 2015, 18(11): 1886-1888. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMGY201511031.htm
[14] 张亚豪, 张扬辉, 陈鹏磊, 等. 中国非ST段抬高型急性冠状动脉综合征患者PCI术后早期应用依洛尤单抗的有效性及安全性研究[J]. 临床心血管病杂志, 2022, 38(8): 623-630. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.08.006
[15] Rashid M, Fischman DL, Gulati M, et al. Temporal trends and inequalities in coronary angiography utilization in the management of non-ST-Elevation acute coronary syndromes in the US[J]. Sci Rep, 2019, 9(1): 240. doi: 10.1038/s41598-018-36504-y
[16] Dakhil ZA, Farhan HA. Non-ST elevation acute coronary syndromes; clinical landscape, management strategy and in-hospital outcomes: an age perspective[J]. Egypt Heart J, 2021, 73(1): 33. doi: 10.1186/s43044-021-00155-8
[17] Leng W, Yang J, Fan X, et al. Behalf CAMI Registry investigators. Contemporary invasive management and in-hospital outcomes of patients with non-ST-segment elevation myocardial infarction in China: Findings from China Acute Myocardial Infarction(CAMI)Registry[J]. Am Heart J, 2019, 215: 1-11. doi: 10.1016/j.ahj.2019.05.015
[18] Khalil M, Maqsood MH, Basir MB, et al. Meta-analysis on invasive versus conservative strategy in patients older than seventy years with Non-ST elevation myocardial infarction[J]. Am J Cardiol, 2023, 186: 66-70. doi: 10.1016/j.amjcard.2022.10.011
[19] Hu M, Li X, Yang Y. Invasive versus conservative management of NSTEMI patients aged ≥ 75 years[J]. Arq Bras Cardiol, 2023, 120(6): e20220658. doi: 10.36660/abc.20220658
[20] Abusnina W, Radaideh Q, Al-Abdouh A, et al. Routine invasive strategy in elderly patients with non-ST elevation acute coronary syndrome: an updated systematic review and meta-analysis of randomized trials[J]. Curr Probl Cardiol, 2022, 47(10): 101304. doi: 10.1016/j.cpcardiol.2022.101304
[21] Sanchis J, Bueno H, Miñana G, et al. Effect of routine invasive vs conservative strategy in older adults with frailty and non-st-segment elevation acute myocardial infarction: a randomized clinical trial[J]. JAMA Intern Med, 2023, 183(5): 407-415. doi: 10.1001/jamainternmed.2023.0047
[22] Gragnano F, Capolongo A, Terracciano F, et al. Le nuove frontiere della terapia antiaggregante: terapia guidata e de-escalation dopo sindrome coronarica acuta o rivascolarizzazione coronarica percutanea[J]. G Ital Cardiol(Rome), 2023, 24(2): 99-109.
-

图(11)
表(1)
计量
- 文章访问数: 1667
- PDF下载数: 3
- 施引文献: 0