
The application value of thioredoxin-interacting protein and inflammasome 3 in chronic heart failure
-
摘要: 目的 分析硫氧还蛋白相互作用蛋白(TXNIP)、炎症小体3(NLRP3)与心力衰竭(心衰)患者再住院率、活动耐量间的关系。 方法 入选患者分为对照组(60例)、射血分数保留组(50例)、射血分数中间组(50例)和射血分数降低组患者(40例)。检测各组患者血浆中TXNIP、NLRP3、BNP的表达水平;记录患者心脏彩超、6 min步行试验结果。分析血清中TXNIP、NLRP3的表达水平是否和心脏功能、患者活动耐力和心衰的再入院率相关。 结果 各组年龄和基础病史间无明显差异。随访期间随着射血分数的减低和患者活动耐力降低,血清中TXNIP和NLRP3的表达水平明显升高(P<0.001)。回归分析显示TXNIP和NLRP3是心衰患者再发住院的独立危险因素(P<0.001)。TXNIP和NLRP3预测心衰患者再住院曲线下面积分别为0.815、0.882。 结论 TXNIP和NLRP3的表达水平随射血分数和活动耐量的减低逐渐增加,TXNIP和NLRP3是可用于心衰患者再入院的预测因素。
-
关键词:
- 心力衰竭 /
- 再住院次数 /
- 硫氧还蛋白相互作用蛋白
Abstract: Objective To analyze the roles of thioredoxin interacting protein(TXNIP) and inflammatory body 3(NLRP3) in patients with heart failure(CHF). Methods The patients were divided into control group(60 cases), ejection fraction retention group(50 cases), intermediate ejection fraction group(50 cases) and reduced ejection fraction group(40 cases). The expression levels of TXNIP, NLRP3 and BNP in plasma were detected. The results of heart color ultrasound and 6 min walking test were recorded. The TXNIP and NLRP3 in serum were detected. Results During the follow-up period, the expression levels of TXNIP and NLRP3 increased significantly with the decrease of ejection fraction and activity endurance(P < 0.001). Regression analysis showed that TXNIP and NLRP3 were independent risk factors for rehospitalization in patients with heart failure(P < 0.001). The area under curve of TXNIP and NLRP3 in ROC curve were 0.815 and 0.882, respectively. Conclusion The expression levels of TXNIP and NLRP3 increased with the decrease of ejection fraction and activity tolerance, and TXNIP and NLRP3 could be used as predicators of readmission in patients with heart failure.-
Key words:
- heart failure /
- number of readmissions /
- thioredoxin-interacting protein
-

-
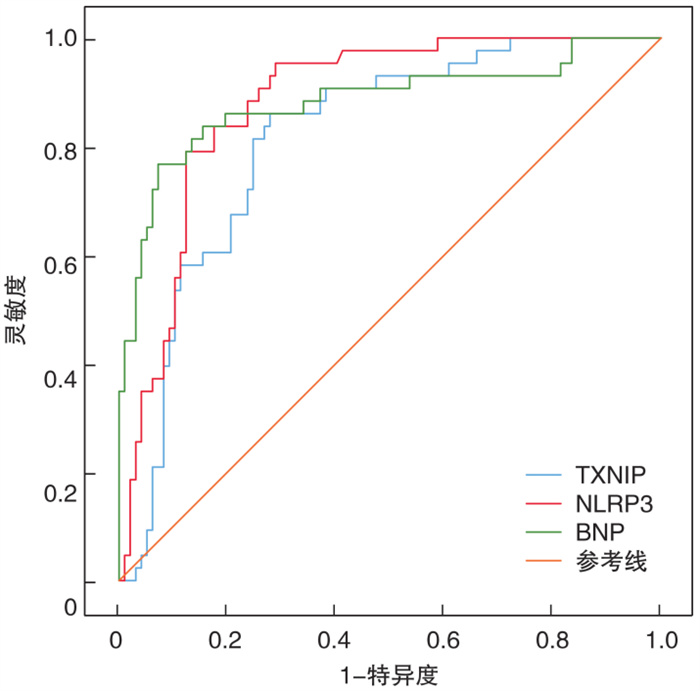
图 1 血浆中TXNIP、NLRP3、BNP预测心衰患者再入院的ROC曲线
Figure 1. ROC curve of plasma TXNIP, NLRP3, and BNP in predicting readmission in heart failure
表 1 患者的基本信息
Table 1. Basic information of patients
例(%), X±S 项目 对照组(60例) HFpEF组(50例) HFmEF组(50例) HFrEF组(40例) P F/χ2 MS 年龄/岁 66.33±6.28 68.16±6.12 67.06±7.00 68.03±5.21 0.390 1.01 38.98 女性 31(51.7) 23(46.0) 25(50.0) 18(45.0) 0.890 0.61 - 基础疾病 高血压病 39(65.0) 31(62.0) 33(66.0) 22(55.0) 0.710 1.39 - 糖尿病 25(41.7) 24(53.3) 18(36.0) 16(40.0) 0.260 4.01 - 冠心病 26(43.3) 20(40.0) 21(42.0) 16(40.0) 0.890 0.17 - 心房颤动 21(42.0) 18(36.0) 18(36.0) 11(27.5) 0.570 2.04 - 口服药物 螺内酯/(mg/d) 0 4.40±7.60 9.80±9.99 14.00±10.33 <0.001 30.47 1 849.00 美托洛尔/(mg/d) 6.33±15.06 9.50±14.39 20.33±18.81 18.41±15.67 <0.001 9.23 2 377.00 达格列净/(mg/d) 1.67±3.76 1.82±3.87 3.4±4.79 5.50±5.04 <0.001 7.68 144.20 沙库巴曲缬沙坦/(mg/d) 8.33±27.87 9.00±21.88 22.00±35.23 41.25±49.21 <0.001 9.32 6 548.00 白细胞/(×109/L) 7.48±1.55 7.29±1.57 7.29±1.42 7.08±1.72 0.670 0.52 1.26 肌酐/(μmol/L) 60.14±48.54 61.80±12.27 65.27±18.64 61.45±15.94 0.440 0.90 251.00 ALT/(U/L) 35.64±6.29 34.93±5.64 35.34±5.57 34.79±6.21 0.880 0.22 7.69 注:ALT:谷丙转氨酶。  下载: 导出CSV
下载: 导出CSV
表 2 各组患血清及心脏彩超指标比较
Table 2. Comparison of serum indicators and cardiac color ultrasound indicators of patients in each group
X±S 指标 对照组(60例) HFpEF组(50例) HFmEF组(50例) HFrEF组(40例) P F MS TXNIP/(pg/mL) 32.24±5.78 44.58±7.92 51.50±7.95 60.90±11.57 <0.001 122.64 6628.00 NLRP3/(pg/mL) 33.79±7.76 39.97±7.64 51.35±8.47 56.53±7.92 <0.001 84.50 5336.00 LDL/(mmol/L) 2.29±0.47 2.30±0.43 2.41±0.53 2.34±0.36 0.510 0.77 0.16 胆固醇/(mmol/L) 4.09±0.64 4.03±0.55 4.07±0.49 4.06±0.67 0.940 0.13 0.05 CRP/(mg/L) 0.59±0.09 0.56±0.08 0.58±0.11 0.59±0.11 0.260 1.35 0.01 BNP/(pg/mL) 27.03±7.05 34.80±11.76 37.63±11.23 42.60±11.09 <0.001 20.38 2152.00 LVEDD/mm 46.45±1.29 46.71±1.47 47.32±1.50 48.55±1.78 <0.001 18.91 42.34 LVESD/mm 30.13±1.94 31.52±1.34 34.44±1.28 38.14±2.19 <0.001 198.73 585.40 LVEF/% 58.82±3.85 54.67±1.93 47.84±2.41 37.82±3.14 <0.001 491.91 4275.00
下载: 导出CSV
表 3 患者6 min步行试验中血浆TXNIP、NLRP3表达
Table 3. Expression levels of TXNIP and NLRP3 in the plasma of patients during the six-minute walking distance
pg/mL, X±S 指标 <150 m(22例) 150~450 m(75例) >450 m(43例) P F MS TXNIP 56.18±8.82 49.27±9.97 44.05±10.07 0.001 11.32 1094.0 NLRP3 57.88±8.19 49.86±9.99 45.00±9.69 0.001 13.03 1211.0 BNP 53.28±21.32 47.60±15.62 45.17±15.33 0.180 1.76 480.1
下载: 导出CSV
表 4 再住院组和无再住院组比较
Table 4. Data between the readmission and the non-rehospitalization groups
X±S 指标 再住院组(43例) 未再住院组(97例) P t TXNIP/(pg/mL) 57.05±7.09 45.51±9.15 <0.001 8.090 NLRP3/(pg/mL) 58.24±6.83 44.54±9.06 <0.001 8.850 BNP/(pg/mL) 50.29±36.54 36.54±9.54 <0.001 7.650 LVEDD/mm 48.26±1.75 47.13±1.64 0.010 3.660 LVESD/mm 35.90±33.81 33.81±2.94 <0.001 3.860 LVEF/% 44.35±6.94 48.38±7.52 0.030 2.990 肌酐/(μmol/L) 62.48±16.83 63.15±15.42 0.819 0.229 CRP/(mg/L) 0.58±0.12 0.58±0.09 0.922 0.098 LDL/(mmol/L) 2.32±0.40 2.25±0.45 0.340 0.950 总胆固醇/(mmol/L) 3.93±0.51 3.95±0.52 0.290 0.770
下载: 导出CSV
表 5 心衰再住院的单因素logistic回归分析
Table 5. Univariate logistic regression analysis of rehospitalization in patients with heart failure
变量 B SE Wald χ2 P OR 95%CI LVEDD 0.231 0.220 1.120 0.290 1.12 0.81~1.93 LVESD 0.132 0.214 0.379 0.538 1.16 0.75~1.74 LVEF -0.090 0.074 0.016 0.901 0.92 0.86~1.15 BNP 0.140 0.030 28.080 <0.001 1.15 1.12~1.31 LDL 0.390 0.515 0.580 0.450 1.28 0.54~4.06 总胆固醇 -0.110 0.360 0.087 0.770 0.89 0.44~1.82 TXNIP 0.150 0.030 29.980 <0.001 1.16 1.14~1.29 NLRP3 0.201 0.030 35.060 <0.001 1.23 1.13~1.31
下载: 导出CSV
-
[1] Pagel PS, Tawil JN, Boettcher BT, et al. Heart failure with preserved ejection fraction: A comprehensive review and update of diagnosis, pathophysiology, treatment, and perioperative implications[J]. J Cardiothorac Vasc Anesth, 2021, 35(6): 1839-1859. doi: 10.1053/j.jvca.2020.07.016
[2] Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary[J]. J Am Coll Cardiol, 2022, 79(17): 1757-1780. doi: 10.1016/j.jacc.2021.12.011
[3] Tanai E, Frantz S. Pathophysiology of heart failure[J]. Compr Physiol, 2015, 6(1): 187-214.
[4] Fu J, Wu H. Structural mechanisms of NLRP3 inflammasomeassembly and activation[J]. Annu Rev Immunol, 2023, 41: 301-316. doi: 10.1146/annurev-immunol-081022-021207
[5] Zheng Y, Xu L, Dong N, et al. NLRP3 inflammasome: the rising star in cardiovascular diseases[J]. Front Cardiovasc Med, 2022, 9: 927061. doi: 10.3389/fcvm.2022.927061
[6] Wang C, Yang T, Xiao J, et al. NLRP3 inflammasome activation triggers gasdermin D-independent inflammation[J]. Sci Immunol, 2021, 6(64): eabj3859. doi: 10.1126/sciimmunol.abj3859
[7] Paik S, Kim JK, Silwal P, et al. An update on the regulatory mechanisms of NLRP3 inflammasome activation[J]. Cell Mol Immunol, 2021, 18(5): 1141-1160. doi: 10.1038/s41423-021-00670-3
[8] Liu Y, Shu J, Liu T, et al. Nicorandil protects against coronary microembolization-induced myocardial injury by suppressing cardiomyocytepyroptosis via the AMPK/TXNIP/NLRP3 signaling pathway[J]. Eur J Pharmacol, 2022, 936: 175365. doi: 10.1016/j.ejphar.2022.175365
[9] Chen ZQ, Zhou Y, Chen F, et al. miR-200a-3p attenuates coronary microembolization-induced myocardial injury in rats by inhibiting TXNIP/NLRP3-mediated cardiomyocytepyroptosis[J]. Front Cardiovasc Med, 2021, 8: 693257. doi: 10.3389/fcvm.2021.693257
[10] 中华医学会心血管病学分会心力衰竭学组, 中国医师协会心力衰竭专业委员会, 中华心血管病杂志编辑委员会. 中国心力衰竭诊断和治疗指南2018[J]. 中华心血管病杂志, 2018, 46(10): 760-789. doi: 10.3760/cma.j.issn.0253-3758.2018.10.004
[11] G-CHF Investigators, Joseph P, Roy A, et al. Global variations in heart failure etiology, management, and outcomes[J]. JAMA, 2023, 329(19): 1650-1661. doi: 10.1001/jama.2023.5942
[12] Rashid S, Gulfam A, Noor TA, et al. Anxiety and depression in heart failure: an updated review[J]. Curr Probl Cardiol, 2023, 48(11): 101987. doi: 10.1016/j.cpcardiol.2023.101987
[13] Sreenivasan J, Khan MS, Ochani RK, et al. Major depression and anxiety among patients hospitalized with heart failure[J]. Am J Cardiol, 2021, 142: 153-155. doi: 10.1016/j.amjcard.2020.12.053
[14] 王敢, 钟江华. NLRP3炎性小体在慢性心力衰竭中的作用与机制[J]. 临床心血管病杂志, 2023, 39(8): 591-596. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2023.08.005
[15] Del Buono MG, Crea F, Versaci F, et al. NLRP3 Inflammasome: a new promising therapeutic target to treat heart failure[J]. J Cardiovasc Pharmacol, 2021, 77(2): 159-161. doi: 10.1097/FJC.0000000000000946
[16] Ma Q, Wang M, Li L, et al. Jieduquyudecoction mitigates monocrotaline-induced right-sided heart failure associated with pulmonary artery hypertension by inhibiting NLRP3 inflammasome in rats[J]. J Ethnopharmacol, 2023, 313: 116556. doi: 10.1016/j.jep.2023.116556
[17] Zhang X, Yao Y, Zhang Y, et al. Prognostic value of patient-reported outcomes in predicting 30 day all-cause readmission among older patients with heart failure[J]. ESC Heart Fail, 2022, 9(5): 2840-2850. doi: 10.1002/ehf2.13991
[18] Cheng X, Zhao H, Wen X, et al. NLRP3-inflammasome inhibition by MCC950 attenuates cardiac and pulmonary artery remodelling in heart failure with preserved ejection fraction[J]. Life Sci, 2023, 333: 122185. doi: 10.1016/j.lfs.2023.122185
[19] Kayhan Kocak FO, Sahin S, Tașkıran E, et al. Frequency and risk factors of re-hospitalization in geriatric inpatient wards: a multicenter retrospective analysis[J]. Exp Aging Res, 2023, 49(1): 70-82. doi: 10.1080/0361073X.2022.2041323
[20] Ritti-Dias RM, Quintella B. The Six-Minute Step Test as an Alternative for Functional Capacity Assessment in Patients with Cardiovascular Diseases[J]. Arq Bras Cardiol, 2021, 116(5): 896-897. doi: 10.36660/abc.20210252
-
图(1)
表(5)
计量
- 文章访问数: 728
- PDF下载数: 56
- 施引文献: 0