
The application value of platelet/lymphocyte ratio, fibrinogen/albumin ratio in the prognosis evaluation of patients with myocardial infarction with non-obstructive coronary arteries
-
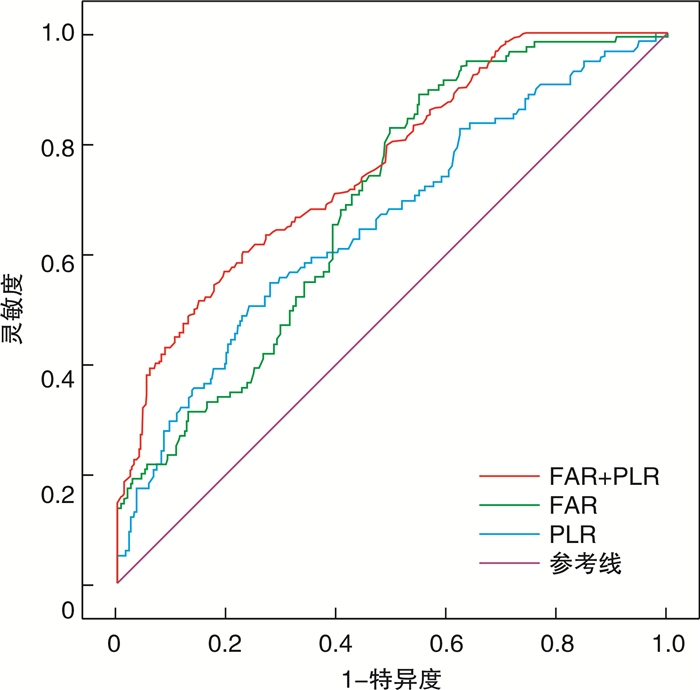
摘要: 目的 评估入院时血小板/淋巴细胞比值(PLR)、纤维蛋白原/白蛋白比值(FAR)及两者联合在冠状动脉非阻塞性心肌梗死(MINOCA)患者预后的应用价值。方法 回顾性收集2018年5月—2022年12月于沧州市人民医院诊断为MINOCA的438例患者的临床资料。根据随访期间是否发生主要不良心脑血管事件(MACCE),将患者分为MACCE组(116例)和非MACCE组(322例)。采用logistic回归分析MINOCA患者预后的影响因素。运用ROC曲线评估PLR、FAR及两者联合对随访期间MACCE的预测价值。结果 两组男性占比、糖尿病占比、淋巴细胞、中性粒细胞、白蛋白、高密度脂蛋白胆固醇、尿酸、左心室射血分数、PLR及FAR比较存在显著差异(均P<0.05)。多因素logistic回归分析显示,中性粒细胞、尿酸、左心室射血分数、PLR、FAR的升高和糖尿病均为MINOCA患者MACCE的危险因素。PLR、FAR及两者联合预测MACCE的ROC曲线下面积(AUC)分别为0.656、0.691、0.762。结论 PLR和FAR是MINOCA患者MACCE的影响因素。
-
关键词:
- 冠状动脉非阻塞性心肌梗死 /
- 血小板/淋巴细胞比值 /
- 纤维蛋白原/白蛋白比值 /
- 主要不良心脑血管事件 /
- 相关性
Abstract: Objective The aim of this study was to evaluate the prognostic value of platelet/lymphocyte ratio(PLR), fibrinogen/albumin ratio(FAR) and their combination in patients with myocardial infarction with non-obstructive coronary arteries(MINOCA).Methods The clinical data of 438 patients diagnosed with MINOCA in Cangzhou People 's Hospital from May 2018 to December 2022 were retrospectively collected. Patients were divided into MACCE group(n=116) and non-MACCE group(n=322) according to whether major adverse cardiovascular and cerebrovascular events(MACCE) occurred during follow-up. Logistic regression was used to analyze the prognostic factors of MINOCA patients. ROC curve was used to evaluate the predictive value of PLR, FAR and their combination for MACCE during follow-up.Results There were significant differences in the proportion of diabetes, lymphocytes, neutrophils, albumin, high-density lipoprotein cholesterol, uric acid, left ventricular ejection fraction, PLR and FAR between the two groups(all P < 0.05). Multivariate logistic regression analysis showed that diabetes, neutrophils, uric acid, left ventricular ejection fraction, PLR and FAR were independent influencing factors of MACCE in MINOCA patients. The area under the ROC curve(AUC) of PLR, FAR and their combination in predicting MACCE was 0.656, 0.691 and 0.762, respectively.Conclusion High PLR and high FAR are associated with an increased risk of MACCE in MINOCA patients, which may help to improve the clinical management strategy of MINOCA patients. -

-
表 1 两组患者基线临床资料比较
Table 1. General data
例(%), X±S, M(P25, P75) 项目 MACCE组(116例) 非MACCE组(322例) 检验值 P值 男性 65(56.0) 218(67.7) 5.077 0.024 年龄/岁 58.87±10.78 60.51±11.13 1.371 0.171 吸烟 38(32.8) 101(31.4) 0.076 0.782 高血压病 73(62.9) 195(60.7) 0.171 0.679 糖尿病 28(24.1) 44(13.7) 6.810 0.009 脑血管疾病 9(7.8) 45(14.0) 2.958 0.085 白细胞/(×109/L) 7.85(6.02,10.07) 7.17(5.93,9.27) 1.690 0.091 血小板/(×109/L) 227.32±67.40 219.53±61.06 0.961 0.282 淋巴细胞/(×109/L) 1.40±0.75 1.74±0.71 4.435 <0.001 中性粒细胞/(×109/L) 7.16(4.91,8.23) 5.04(3.68,6.83) 4.242 <0.001 C反应蛋白/(mg/L) 8.10(0.62,26.62) 2.80(0.52,12.62) 1.538 0.069 白蛋白/(g/L) 38.92±4.19 41.99±4.51 3.201 <0.001 纤维蛋白原/(g/L) 4.17±1.07 3.32±0.82 0.634 0.660 D-二聚体/(ng/mL) 112(58,218) 100(57,203) 0.851 0.357 PLR 159.34(141.06,226.51) 142.25(105.98,217.11) 5.772 <0.001 FAR 11.32±2.16 8.53±1.51 3.701 <0.001 总胆固醇/(mmol/L) 4.51±1.19 4.27±1.07 1.896 0.059 甘油三酯/(mmol/L) 1.09(0.92,1.87) 1.27(0.90,1.78) 0.009 0.993 高密度脂蛋白胆固醇/(mmol/L) 1.19±0.29 1.27±0.38 2.337 0.020 低密度脂蛋白胆固醇/(mmol/L) 2.67±0.94 2.46±0.91 1.938 0.053 肌酐/(μmol/L) 64(55,77) 62(54,85) 0.848 0.397 尿酸/(μmol/L) 342.91±55.98 303.13±69.91 2.230 0.027 空腹血糖/(mmol/L) 5.94(5.19,8.18) 5.57(5.19,6.78) 0.172 0.864 糖化血红蛋白/% 5.8(5.5,6.3) 5.7(5.5,6.3) 0.317 0.751 左心室射血分数/% 55.5(51.5,61.0) 59.0(56.0,62.0) 4.843 <0.001 肌钙蛋白I/(μg/L) 0.62±0.15 0.58±0.13 1.670 0.097  下载: 导出CSV
下载: 导出CSV
表 2 MINOCA患者发生MACCE的危险因素分析
Table 2. Logistic regression analysis
变量 单因素分析 多因素分析 P值 OR(95%CI) P值 OR(95%CI) 男性 0.025 1.008(1.005~1.010) 0.276 0.706(0.377~1.322) 糖尿病 0.010 2.046(1.079~3.881) 0.028 1.910(1.282~2.419) 淋巴细胞 <0.001 0.443(0.306~0.641) 0.716 0.882(0.449~1.734) 高密度脂蛋白胆固醇 0.040 0.516(0.275~0.970) 0.138 0.574(0.276~1.194) 白蛋白 <0.001 0.972(0.958~0.987) 0.060 0.973(0.946~1.001) 中性粒细胞 <0.001 1.197(1.099~1.303) 0.041 1.109(1.004~1.224) 尿酸 0.041 1.005(1.002~1.008) 0.049 1.003(1.000~1.005) 左心室射血分数 <0.001 1.020(1.080~1.039) <0.001 1.009(0.974~1.146) PLR <0.001 1.008(1.045~1.225) 0.017 1.007(1.001~1.013) FAR <0.001 1.240(1.015~1.063) <0.001 1.025(1.045~1.073)
下载: 导出CSV
-
[1] Worner F, Cequier A, Alfredo B, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation[J]. Euro Heart J, 2012, 33(1): 2569-2619.
[2] Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction(2018)[J]. J Am Coll Cardiol, 2018, 72(18): 2231-2264. doi: 10.1016/j.jacc.2018.08.1038
[3] Giampaolo N, Giancarla S, Filippo C. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management[J]. Euro Heart J, 2023, 10(8): 475.
[4] Pasupathy S, Air T, Dreyer RP, et al. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. [J]. Circulation, 2015, 132(19): 861-870.
[5] Eggers KM, Baron T, Hjort M, et al. Clinical and prognostic implications of C-reactive protein levels in myocardial infarction with nonobstructive coronary arteries[J]. Clin Cardiol, 2021, 44(7): 1019-1027. doi: 10.1002/clc.23651
[6] Gürdal A, Keskin K, Siǧirci S, et al. Prognostic value of the neutrophil-to-lymphocyte ratio in patients with myocardial infarction with non-obstructive coronary arteries[J]. Angiology, 2020, 71(9): 812-816. doi: 10.1177/0003319720938621
[7] Paolisso P, Foà A, Bergamaschi L, et al. Hyperglycemia, inflammatory response and infarct size in obstructive acute myocardial infarction and MINOCA[J]. Cardiovasc Diabetol, 2021, 20(1): 33. doi: 10.1186/s12933-021-01222-9
[8] Cheema AN, Yanagawa B, Verma S, et al. Myocardial infarction with nonobstructive coronary artery disease(MINOCA): a review of pathophysiology and management[J]. Curr Opin Cardiol, 2021, 36(5): 589-596. doi: 10.1097/HCO.0000000000000886
[9] Wang P, Yuan D, Zhang C, et al. High fibrinogen-to-albumin ratio with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention: 5-year findings from a large cohort[J]. Cardiovasc Diabetol, 2022, 21(1): 46. doi: 10.1186/s12933-022-01477-w
[10] Kang Y, Zhu X, Lin Z, et al. Compare the diagnostic and prognostic value of MLR, NLR and PLR in CRC Patients[J]. Clin Lab, 2021, 67(9): 110.
[11] Fang T, Wang Y, Yin X, et al. Diagnostic sensitivity of NLR and PLR in early diagnosis of gastric cancer[J]. J Immunol Res, 2020, 2020(5): 1-9.
[12] 徐亚东, 张磊, 努尔夏提·阿布力米提, 等. 术前NLR和PLR联合各共识在胰腺分支型导管内乳头状肿瘤手术决策中的价值[J]. 中华普通外科杂志, 2017, 32(9): 733-737. doi: 10.3760/cma.j.issn.1007-631X.2017.09.004
[13] Köse N, Yıldırım T, Akın F, et al. Prognostic role of NLR, PLR, and LMR in patients with pulmonary embolism[J]. Bosn J Basic Med Sci, 2020, 20(2): 248-253.
[14] 范青, 满其航, 王玉. 血小板/淋巴细胞与重型再生障碍性贫血患者血液学反应的关联性研究[J]. 临床血液学杂志, 2023, 36(10): 746-750, 754. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202310012.htm
[15] Singh T, Chapman AR, Dweck MR, et al. MINOCA: a heterogenous group of conditions associated with myocardial damage[J]. Heart, 2021, 107(18): 1458-1464. doi: 10.1136/heartjnl-2020-318269
[16] Abdu FA, Mohammed AQ, Liu L, et al. Myocardial Infarction with Nonobstructive Coronary Arteries(MINOCA): A Review of the Current Position[J]. Cardiology, 2020, 145(9): 543-552. doi: 10.1159/000509100
[17] 费思凡, 贾方, 张胜. 炎症在冠状动脉非阻塞性心肌梗死中的作用[J]. 中国动脉硬化杂志, 2023, 31(6): 533-538. https://www.cnki.com.cn/Article/CJFDTOTAL-KDYZ202306011.htm
[18] Horie T, Sugiyama T, Kanaji Y, et al. Serial assessment of pericoronary adipose tissue inflammation in a patient with MINOCA potentially complicated with vasospasm[J]. CJC Open, 2021, 3(2): 204-206. doi: 10.1016/j.cjco.2020.10.001
[19] Boag SE, Das R, Shmeleva EV, et al. T lymphocytes and fractalkine contribute to myocardial ischemia/reperfusion injury in patients[J]. J Clin Invest, 2015, 125(8): 3063-3076. doi: 10.1172/JCI80055
[20] Rock KL, Kono H. The inflammatory response to cell death[J]. Annu Rev Pathol, 2008, 3: 99-126. doi: 10.1146/annurev.pathmechdis.3.121806.151456
[21] 韩良富, 卞晓洁, 潘赟, 等. 血小板参数在急性心肌梗死临床评估中的作用[J]. 中华急诊医学杂志, 2016, 25(3): 349-355. doi: 10.3760/cma.j.issn.1671-0282.2016.03.019
[22] 孙静, 任法新, 孙晓健, 等. 血小板-淋巴细胞聚集体和血小板/淋巴细胞比值在预测急诊经皮冠状动脉介入治疗术后心肌无复流中的作用[J]. 中国循环杂志, 2018, 33(9): 869-872. doi: 10.3969/j.issn.1000-3614.2018.09.010
[23] 刘芳, 李彩霞, 韩新, 等. 不同MAPP量对心脏瓣膜置换手术患者肺功能保护及凝血功能的影响[J]. 临床血液学杂志, 2023, 36(12): 878-883. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202312008.htm
[24] Libby P, Pasterkamp G, Crea F, et al. Reassessing the mechanisms of acute coronary syndromes[J]. Circ Res, 2019, 124(1): 150-160. doi: 10.1161/CIRCRESAHA.118.311098
[25] 张春亚, 姚漫, 张凯, 等. 冠心病患者血小板和淋巴细胞比值与冠脉斑块稳定性及预后的相关性研究[J]. 血栓与止血学, 2021, 27(1): 53-54. doi: 10.3969/j.issn.1009-6213.2021.01.021
[26] 孙亚召, 孙东旭, 黄淑田. 血小板与淋巴细胞比值对冠状动脉病变及介入治疗预后的预测价值[J]. 中华老年心脑血管病杂志, 2019, 21(5): 490-493. doi: 10.3969/j.issn.1009-0126.2019.05.011
[27] Cakmak G, Zdemir K, Mantolu B, et al. Mortality in acute arterial mesenteric ischemia: a single-center experience[J]. Sakarya Tip Dergisi, 2021(3): 110.
[28] 陈桤璐, 卢志贤, 刘敏, 等. 血清hs-cTnT、PCT、FIB与血小板聚集率在冠心病中的表达及意义[J]. 临床血液学杂志, 2023, 36(12): 873-877. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXZ202312007.htm
[29] China L, Skene SS, Bennett K, et al. ATTIRE: Albumin to prevent infection in chronic liver failure: study protocol for an interventional randomised controlled trial[J]. BMJ Open, 2018, 8(10): e023754. doi: 10.1136/bmjopen-2018-023754
[30] Garcia-Martinez R, Caraceni P, Bernardi M, et al. Albumin: pathophysiologic basis of its role in the treatment of cirrhosis and its complications[J]. Hepatology, 2013, 58(5): 1836-1846. doi: 10.1002/hep.26338
[31] Yoshioka G, Tanaka A, Nishihira K, et al. Prognostic impact of serum albumin for developing heart failure remotely after acute myocardial infarction[J]. Nutrients, 2020, 12(9): 2637. doi: 10.3390/nu12092637
[32] Wang P, Yuan D, Zhang C, et al. High fibrinogen-to-albumin ratio with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention: 5-year findings from a large cohort[J]. Cardiovasc Diabetol, 2022, 21(1): 46. doi: 10.1186/s12933-022-01477-w
[33] Çetin M, Erdoǧan T, Kırış T, et al. Predictive value of fibrinogen-to-albumin ratio in acute coronary syndrome[J]. Herz, 2020, 45(Suppl 1): 145-151.
[34] Liu G, Fan CM, Guo H, et al. Fibrinogen-to-albumin ratio predicts long-term outcomes for patients with ST-elevation myocardial infarction and multivessel disease: A prospective observational cohort study[J]. Exp Ther Med, 2021, 21(5): 465. doi: 10.3892/etm.2021.9896
-
图(1)
表(2)
计量
- 文章访问数: 483
- PDF下载数: 65
- 施引文献: 0