
The application of shockwave balloon in percutaneous coronary intervention for severe coronary artery calcification
-
摘要: 目的 观察新型冲击波球囊碎石技术在冠状动脉(冠脉)严重钙化病变中的治疗效果。方法 根据冠脉造影结果以及腔内影像学指导,将25例患者分为冲击波组(15例)和对照组(10例)。其中,冲击波组12例采用光学相干断层成像(optical coherence tomography,OCT)检查,3例采用血管内超声(intravascular ultrasound,IVUS)检查;对照组6例行OCT检查,4例行IVUS检查。比较两组患者术中使用耗材情况、手术曝光时间、斑块负荷、最小管腔直径、最小管腔面积、支架内最小管腔面积及支架膨胀率,并记录术后和半年随访期间发生的主要心血管不良事件。结果 冲击波组术中使用耗材数量明显减少,曝光时间明显缩短[(120.34±7.05) min vs(80.66±6.19) min,P < 0.05]。两组患者术后的斑块负荷、最小管腔直径和最小管腔面积均较术前明显改善(均P < 0.05)。与对照组比较,冲击波组术后支架内最小管腔面积[(9.23±1.37) mm2 vs (11.89±3.25) mm2,P < 0.05]和支架膨胀率[(78.31±3.55)% vs (89.22±2.65)%,P < 0.05]改善更为明显。所有患者术后以及半年随访期间均未发生主要心血管不良事件。结论 冲击波球囊导管技术在冠脉严重钙化病变中应用是安全有效的。Abstract: Objective To evaluate the therapeutic effect of a new type of shockwave lithotripsy in the treatment of severe coronary calcification.Methods Based on the results of coronary angiography and guidance of intracavitary imaging, 25 patients were divided into the shockwave group(n=15) and control group(n=10). In the shockwave group, OCT was performed in 12 cases and IVUS in 3 cases. In the control group, OCT was performed in 6 cases and IVUS in 4 cases. The use of consumables during the operation, surgical exposure time, plaque burden, minimal lumen diameter, minimal lumen area, minimal lumen area inside the stent, and stent expansion rate were compared between the two groups. Major cardiovascular adverse events were recorded after surgery and during the 6-month follow-up.Results In the shockwave group, the amount of consumables use during operation was significantly reduced and the exposure time was significantly shortened[(120.34±7.05) min vs (80.66±6.19) min, P < 0.05]. The plaque burden, minimum lumen diameter, and minimum lumen area after surgery were significantly improved compared to those before operation in both groups(all P < 0.05). Compared with the control group, the minimum lumen area in the stent[(9.23±1.37) mm2vs (11.89±3.25) mm2, P < 0.05] and stent expansion rate[(78.31±3.55)% vs (89.22±2.65)%, P < 0.05] improved more significantly in the shockwave group. There was no major cardiovascular adverse events occurred in all patients after surgery and during the 6-month follow-up.Conclusion It is safe and effective to apply the technique of shockwave balloon catheter in coronary artery severe calcification.
-
Key words:
- coronary calcification /
- shockwave balloon /
- endoluminal imaging
-

-
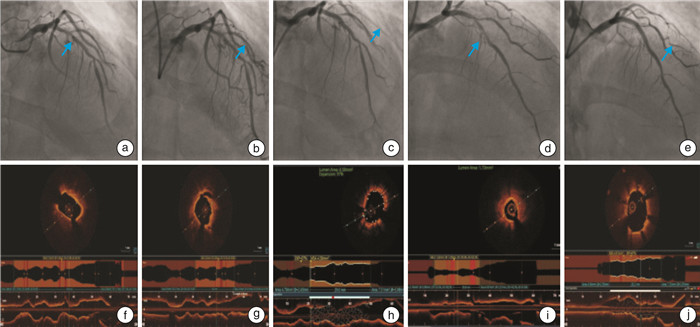
图 1 冠脉造影及PCI术后同步OCT影像
Figure 1. Coronary angiography and synchronous OCT imaging after PCI
表 1 患者一般基线资料
Table 1. General data
例(%), X ± S 项目 对照组(10例) 冲击波组(15例) P 年龄/岁 70.21±6.23 68.67±8.44 0.589 性别 男 6(60.00) 8(53.33) 0.123 女 4(40.00) 7(46.67) 0.323 BMI/(kg/m2) 23.87±5.05 24.95±4.71 0.751 吸烟史 5(50.00) 7(46.67) 0.037 糖尿病 4(40.00) 7(46.67) 0.784 高血压 7(70.00) 10(66.67) 0.322 脑卒中 3(30.00) 6(40.00) 0.303 甲状腺异常 2(20.00) 3(20.00) 0.512 高胆固醇血症 8(80.00) 9(60.00) 0.401 高同型半胱氨酸血症 3(30.00) 4(26.67) 0.551 高尿酸血症 2(20.00) 3(20.00) 0.654 家族史 5(50.00) 7(46.67) 0.425  下载: 导出CSV
下载: 导出CSV
表 2 冠脉钙化病变腔内影像学积分评估
Table 2. Evaluation of intracavitary imaging score in coronary calcification lesions
例(%) 项目 对照组(10例) 冲击波组(15例) χ2 P IVUS参数 1.730 0.052 Ⅰ级(≤90°) 0 0 Ⅱ级(91°~180°) 0 0 Ⅲ级(181°~270°) 3(30.00) 2(13.33) Ⅳ级(≥271°) 1(10.00) 1(6.67) OCT钙化积分 3.440 0.074 3分 2(20.00) 5(33.33) 4分 4(40.00) 7(46.67)
下载: 导出CSV
表 3 PCI术中耗材应用及曝光时间比较
Table 3. Application of consumables and exposure time in PCI
例(%), X ± S 项目 对照组(10例) 冲击波组(15例) χ2/t P 半顺应性球囊 10(100.00) 7(46.67) 8.607 0.062 非顺应性球囊 9(90.00) 0 冲击波球囊 0 15(100.00) 切割球囊 4(40.00) 0 棘突球囊 6(60.00) 0 双导丝 4(40.00) 0 Guidezilla延长导管 6(60.00) 1(6.67) 3.410 < 0.010 曝光时间/min 120.34±7.05 80.66±6.19 6.054 0.019 RA 2(20.00) 0
下载: 导出CSV
表 4 腔内影像学观察指标
Table 4. Indexes of intracavitary imaging
X ± S 项目 对照组(10例) 冲击波组(15例) t P 处理前 处理后 处理前 处理后 钙化斑块长度/mm 33.81±12.58 26.88±12.54 2.131 0.416 斑块负荷/% 87.66±10.71 40.21±6.011) 89.41±9.21 31.33±9.211)2) 0.281 < 0.001 最小管腔直径/mm 2.11±1.72 3.03±1.531) 1.69±1.04 3.43±2.611)2) 1.071 0.023 最小管腔面积/mm2 3.41±1.05 7.22±2.341) 2.25±1.67 9.28±4.131)2) 0.165 < 0.001 术后支架内最小管腔面积/mm2 9.23±1.37 11.89±3.252) 1.872 0.031 术后支架膨胀率/% 78.31±3.55 89.22±2.652) 0.542 < 0.001 与同组处理前比较,1)P < 0.05;与对照组处理后比较,2)P < 0.05。
下载: 导出CSV
-
[1] Moncla Minvielle LH, Briend M, Bosse Y, et al. Calcific aortic valve disease: mechanisms, prevention and treatment[J]. Nat Rev Cardiol, 2023, 20(8): 546-559. doi: 10.1038/s41569-023-00845-7
[2] Rheude T, Fitzgerald S, Allali A, et al. Rotational atherectomy or balloon-based techniques to prepare severely calcified coronary lesions[J]. Cardiovasc Interv, 2022, 15(18): 1864-1874.
[3] 邱翠婷, 朱艳霞, 晋辉, 等. 超声引导下冠状动脉严重钙化病变旋磨后药物洗脱支架置入治疗的临床分析[J]. 中国临床医生杂志, 2022, 50(2): 158-160. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLYS202202010.htm
[4] 杨敏, 林章宇, 丰雷, 等. 冠状动脉造影评估的靶病变钙化程度对接受经皮冠状动脉介入治疗患者手术即刻成功率和长期预后的影响[J]. 中国循环杂志, 2023, 38(12): 1239-1245. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202312001.htm
[5] Torii S, Jinnouchi H, Sakamoto A, et al. Vascular responses to coronary calcification following implantation of newer-generation drug-eluting stents in humans: impact on healing[J]. Eur Heart J, 2020, 41(6): 786-796. doi: 10.1093/eurheartj/ehz850
[6] Maclean E, Sehmi J, Kanaganayagam G, et al. Hypertension attenuates the prognostic value of coronary artery calcification scoring in low-risk patients[J]. Heart, 2021, 107: 977-982. doi: 10.1136/heartjnl-2020-317399
[7] Avital Y, Madar A, Arnon S, et al. Identifcation of coronary calcifcations in optical coherence tomography imaging using deep learning[J]. Sci Rep, 2021, 11(1): 11269. doi: 10.1038/s41598-021-90525-8
[8] 董昊喆, 龚深圳, 单迎光, 等. 冠状动脉旋磨术联合药物涂层球囊治疗冠状动脉严重钙化病变的疗效[J]. 临床心血管病杂志, 2023, 39(2): 108-113. doi: 10.13201/j.issn.1001-1439.2023.02.007
[9] 杨丽睿, 冯婷婷, 赵欣, 等. 经皮冠状动脉腔内冲击波球囊导管成形术治疗冠状动脉钙化病变的研究进展[J]. 中国介入心脏病学杂志[J], 2024, 32(2): 101-107. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXB202402007.htm
[10] Aoi S, Baber U, Kovacic JC, er al. Combined and independent impact of coronary artery calcification and inflammation on risk for adverse cardiovascular events after percutaneous coronary intervention: Results from a large single-center registry[J]. Catheter Cardiovasc Interv, 2020, 96(3): E278-E286.
[11] 赵刚, 葛均波. 新一代国产冠脉液电冲击波球囊导管应用于重度冠脉钙化病变的初步尝试[J]. 中国临床医学, 2022, 29(4): 580-584. https://www.cnki.com.cn/Article/CJFDTOTAL-LCYX202204010.htm
[12] Aziz A, Bhatia G, Pitt M, et al. Intravascular lithotripsy in calcified-coronary lesions: a real-world observational, European multicenter study[J]. Catheter Cardiovasc Interv, 2021, 98(2): 225-235. doi: 10.1002/ccd.29263
[13] Ielasi A, Moscarella E, Testa L, et al. Intravascular lithotripsy for the management of undilatable coronary stent: the SMILE registry[J]. Cardiovasc Revasc Med, 2020, 21(12): 1555-1559. doi: 10.1016/j.carrev.2020.05.020
[14] Sheikh AS, Connolly DL, Abdul F, et al. Intravascular lithotripsy for severe coronary calcification: a systematic review[J]. Minerva Cardiol Angiol, 2023, 71(6): 643-652.
[15] Hill JM, Kereiakes DJ, Shlofmitz RA, et al. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease[J]. JACC, 2020, 22(76): 2635-2646.
[16] Tepe G, Brodmann M, Werner M, et al. Intravascular Lithotripsy for Peripheral Artery Calcification: 30-Day Outcomes From the Randomized Disrupt PAD Ⅲ Trial[J]. JACC Cardiovasc Interv, 2021, 14(12): 1352-1361. doi: 10.1016/j.jcin.2021.04.010
-
图(1)
表(4)
计量
- 文章访问数: 784
- PDF下载数: 698
- 施引文献: 0