
-
摘要: 目的 评估超声心动图引导下封堵继发孔型房间隔缺损(ASD)的有效性和安全性,并确定相关定量指标。方法 回顾性分析我院2020年12月—2023年12月接受经食管超声心动图(TEE)引导下微创封堵116例继发孔型ASD患者。测量放射压缩(X线下封堵伞展开后腰部直径)和超声压缩(术中TEE下封堵伞展开后腰部直径),计算放射压缩比,公式为:压缩比=(封堵伞型号-实际测量值)/封堵伞型号×100%。比较封堵前后心脏结构变化,并分析缺损大小和压缩比之间的相关性。采用二元logistic回归分析评估影响心脏结构变化的因素。并随访术后并发症发生情况。结果 封堵术后,右心系统显著缩小,左心增大,差异均有统计学意义(P < 0.05)。放射压缩比和超声压缩比分别为(23.47±9.36)%和(36.01±8.40)%。压缩比与右室变化和缺损大小均呈负相关(P < 0.05),表明缺损越大,压缩比越小。放射压缩比与超声压缩比之间呈强正相关。术后3例发生封堵器脱落,放射压缩比分别为5.00%、8.33%、5.26%,超声压缩比分别为17.50%、13.89%、7.89%。5例出现残余分流,随访6个月后均消失;1例发生心包填塞,无死亡发生。Logistic回归分析显示,缺损大小是预测右心室结构重塑的独立预测因子(OR=1.273,95%CI 1.148~1.411)。结论 压缩比可作为评估ASD封堵术后安全性的量化指标。较小的压缩比可能提示封堵器脱落风险;缺损大小是右心室结构重塑的预测指标。Abstract: Objective To evaluate the effect and safety of ultrasound-guided closure of secundum atrial septal defect(ASD), and to identify relevant quantitative indicators.Methods A retrospective analysis was conducted on 116 patients with secundum ASD who underwent minimally invasive closure guided by transesophageal echocardiography(TEE) in our hospital from December 2020 to December 2023. We detected the radiation compression(waist diameter after unfolding the occlusion umbrella under X-ray) and ultrasound compression(waist diameter after unfolding the occlusion umbrella under intraoperative TEE), and calculate the radiation compression ratio. The formula is: compression ratio=(occlusion umbrella model-actual measurement value)/occlusion umbrella model × 100. The changes in cardiac structure before and after occlusion were compared, and the correlation between defect size and compression ratio was analyzed. Binary logistic regression analysis was used to evaluate the factors affecting changes in cardiac structure. Postoperative complications were also followed up.Results After the occlusion surgery, the right heart system significantly shrank and the left heart increased, with statistically significant differences(P < 0.05). The radiation compression ratio and ultrasound compression ratio were(23.47 ± 9.36)% and(36.01 ± 8.40)%, respectively. The compression ratio is negatively correlated with right ventricular changes and defect size(P < 0.05), indicating that the larger the defect, the smaller the compression ratio. There is a strong positive correlation between the radiation compression ratio and the ultrasound compression ratio. Three cases of occluder detachment occurred postoperatively, with radiation compression ratios of 5.00%, 8.33%, and 5.26%, and ultrasound compression ratios of 17.50%, 13.89%, and 7.89%, respectively. The 5 cases showed residual shunting, which disappeared after 6 months of follow-up; One case of pericardial tamponade occurred without any deaths. Logistic regression analysis showed that defect size was an independent predictor of right ventricular structural remodeling(OR=1.273, 95%CI 1.148-1.411).Conclusion Compression ratio can be used as a quantitative indicator to evaluate the safety of ASD closure surgery. A smaller compression ratio may indicate a risk of occluder detachment. The size of the defect is a predictive indicator of right ventricular structural remodeling.
-

-
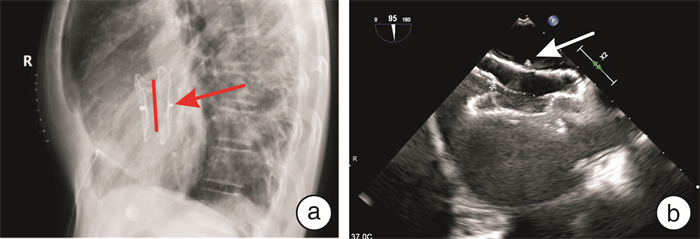
图 1 放射压缩与超声压缩测量方法
Figure 1. Measurement methods of radiation compression and ultrasonic compression
表 1 封堵前后心脏结构及功能指标比较
Table 1. Comparison of cardiac structural and functional indices before and after occlusion
X±S 超声指标 术前 术后出院前 t P LA/mm 35.14±5.89 35.25±6.00 -0.305 0.760 LV/mm 39.77±5.17 42.28±4.58 -6.383 < 0.010 RA1/mm 53.79±7.91 50.02±5.83 6.555 < 0.010 RA2/mm 45.50±7.07 39.79±5.89 9.162 < 0.010 RV/mm 29.61±5.69 25.27±4.01 11.013 < 0.010 MPA/mm 25.52±4.86 24.31±4.48 3.180 < 0.010 MVE/(m/s) 0.85±0.25 0.89±0.27 -1.885 0.062 MVA/(m/s) 0.70±0.20 0.66±0.173 2.163 0.033 MVE/A 1.28±0.50 1.46±0.60 -2.081 0.043 MVe/(m/s) 0.13±0.046 0.11±0.04 3.383 < 0.010 MVa/(m/s) 0.11±0.03 0.19±0.97 -0.881 0.381 MVE/e 7.07±2.67 8.58±3.47 -4.149 < 0.010 LVEF 0.67±0.07 0.69±0.06 2.012 0.047 MVE/A:二尖瓣E/A峰比值;MVE/e:二尖瓣E/e比值。  下载: 导出CSV
下载: 导出CSV
表 2 两组患者临床资料比较
Table 2. Comparison of clinical data between the two groups of patients
例(%), X±S 临床资料 无显著变化组(65例) 显著变化组(51例) P 男 22(33.8) 9(17.6) 0.059 年龄/岁 41.8±12.66 41.2±13.98 0.808 高血压 10(15.4) 4(7.8) 0.205 糖尿病 4(6.2) 0 0.128 吸烟 9(13.8) 3(5.9) 0.154 饮酒 5(7.8) 1(2.0) 0.225 入院收缩压/mmHg 120.83±15.219 120.76±17.516 0.982 入院舒张压/mmHg 74.74±11.278 75.50±11.678 0.724 ASD分型 0.729 单孔型 61(93.8) 47(92.2) 多孔型 4(6.2) 4(7.8) 手术路径 < 0.010 经胸小切口 4(6.2) 18(35.3) 经颈内静脉 46(70.8) 25(49.0) 经股静脉 15(23.1) 8(15.7)
下载: 导出CSV
表 3 两组患者术中主要影像学测量指标
Table 3. Major intraoperative imaging measures in both groups of patients
X±S 术中资料 无显著变化组(65例) 显著变化组(51例) t P 缺损最大径/mm 18.61±6.67 24.67±6.30 -4.974 < 0.010 封堵伞型号/mm 28.75±6.30 34.16±5.75 -4.764 < 0.010 放射压缩/mm 21.92±6.66 26.88±6.34 -4.065 < 0.010 放射压缩比/% 24.67±9.66 21.95±8.82 1.563 0.086 超声压缩/mm 18.29±5.58 22.69±5.74 -4.157 < 0.010 超声压缩比/% 37.25±8.77 34.42±7.71 1.815 0.057 术后住院时间/d 3.51±2.43 5.51±3.78 -3.286 < 0.010
下载: 导出CSV
表 4 RV变化是否显著的影响因素二元logistic回归分析结果
Table 4. Results of binary logistic regression analysis of factors influencing whether the change in RV is significant or not
因素 β Waldχ2 OR 95%CI P 性别 -0.886 2.890 0.412 0.148~1.145 0.089 缺损最大径 0.241 20.903 1.273 1.148~1.411 < 0.010 放射压缩比 0.041 1.316 1.041 0.972~1.116 0.251 超声压缩比 0.050 1.509 1.052 0.970~1.139 0.219 年龄 -0.018 1.093 0.982 0.950~1.016 0.296
下载: 导出CSV
表 5 ASD封堵术后并发症
Table 5. Complications after ASD blockade
并发症 例数 发生时间 放射压缩比 超声压缩比 结局 封堵器脱落 3 术后第4天 5.00% 17.50% 取出脱落封堵器,改为ASD修补术 术后2 h 8.33% 13.89% 取出脱落封堵器,改为ASD修补术 术后第3天 5.26% 7.89% 取出脱落封堵器,换更大封堵器,于RA表面间断缝合两针,固定封堵器。 残余分流 5 术后即刻 25.00% 28.57% 术后即刻下缘探及宽约2 mm残余分流信号;术后1d TTE复查显示自发闭合消失 术后即刻 27.78% 41.67% 术后即刻下腔静脉与三尖瓣之间探及宽约4 mm残余分流;术后14 d发现心包填塞,打开原切口见心脏表面血性纤维组织覆盖,心包腔内吸引出暗红色积血及血凝块;术后3个月近下腔静脉侧(封堵伞下缘)探及宽约4 mm分流。 术后即刻 17.86% 25.00% 术后即刻下缘探及宽约3 mm残余分流信号;术后1d TTE复查显示自发闭合消失 术后即刻 20.00% 33.33% 术后即刻下缘探及宽约2 mm残余分流信号;术后3d TTE复查显示自发闭合消失 术后3个月 28.13% 28.13% 术后3个月封堵器腰部下血流束宽约2 mm;术后6个月未见残余分流。 心包填塞 1 术后14 d 27.78% 41.67% 打开原切口见心脏表面血性纤维组织覆盖,心包腔内吸引出约400 mL暗红色积血及血凝块 心脏组织侵蚀 0 死亡 0
下载: 导出CSV
-
[1] Brida M, Chessa M, Celermajer D, et al. Atrial septal defect in adulthood: a new paradigm for congenital heart disease[J]. Eur Heart J, 2022, 43(28): 2660-2671. doi: 10.1093/eurheartj/ehab646
[2] Qureshi AM, Kenny D. Atrial septal defect closure in patients with pulmonary hypertension: room for punching a hole in the debate[J]. JACC Cardiovasc Interv, 2020, 13(17): 2035-2037. doi: 10.1016/j.jcin.2020.05.023
[3] 许美珍, 肖紫荆, 沈文, 等. 卵圆孔未闭介入封堵术中右心房造影临床评价[J]. 临床心血管病杂志, 2022, 38(5): 365-368. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.05.006
[4] Faletra FF, Saric M, Saw J, et al. Imaging for patient's selection and guidance of LAA and ASD percutaneous and surgical closure[J]. JACC Cardiovasc Imaging, 2021, 14(1): 3-21. doi: 10.1016/j.jcmg.2019.06.032
[5] Akagi T. Current concept of transcatheter closure of atrial septal defect in adults[J]. J Cardiol, 2015, 65(1): 17-25. doi: 10.1016/j.jjcc.2014.09.002
[6] 应岳桦, 楼园青, 徐步云, 等. 塞式封堵器与盘式封堵器对心房颤动患者左心耳封堵术后残余漏的影响[J]. 心电与循环, 2023, 42(5): 500-503.
[7] 中华医学会超声医学分会超声心动图学组. 中国成年人超声心动图检查测量指南[J]. 中华超声影像学杂志, 2016, 25(8): 645-666.
[8] Kim NK, Park SJ, Choi JY. Transcatheter closure of atrial septal defect: does age matter?[J]. Korean Circ J, 2011, 41(11): 633-638. doi: 10.4070/kcj.2011.41.11.633
[9] Oster M, Bhatt AB, Zaragoza-Macias E, et al. Interventional therapy versus medical therapy for secundum atrial septal defect: a systematic review(part 2) for the 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines[J]. J Am Coll Cardiol, 2019, 73(12): 1579-1595. doi: 10.1016/j.jacc.2018.08.1032
[10] 丁铃, 孙子瑞, 毋会芃, 等. 房间隔缺损合并重度三尖瓣反流患者经皮房间隔缺损封堵术后短期疗效观察[J]. 中国循环杂志, 2022, 37(10): 1008-1011.
[11] 阴海霞, 刘爱玲, 周爱香, 等. 应用超声心动图观察房间隔继发孔缺损封堵术后心脏结构与功能的变化[J]. 放射学实践, 2013, 28(6): 689-691.
[12] Akula VS, Durgaprasad R, Velam V, et al. Right ventricle before and after atrial septal defect device closure[J]. Echocardiography, 2016, 33(9): 1381-1388. doi: 10.1111/echo.13250
[13] 李若川, 刘路路, 芮海英, 等. 细胞衰老与心脏重构的研究进展[J]. 中华心血管病杂志, 2021, 49(10): 1048-1052.
[14] Tzifa A, Gordon J, Tibby SM, et al. Transcatheter atrial septal defect closure guided by colour flow Doppler[J]. Int J Cardiol, 2011, 149(3): 299-303. doi: 10.1016/j.ijcard.2010.01.014
[15] 国家卫生健康委员会国家结构性心脏病介入质量控制中心, 国家心血管病中心结构性心脏病介入质量控制中心, 中华医学会心血管病学分会先心病经皮介入治疗指南工作组, 等. 常见先天性心脏病经皮介入治疗指南(2021版)[J]. 中华医学杂志, 2021, 101(38): 3054-3076.
[16] Salmon MK, Hammer KE, Nygaard JV, et al. Left atrial appendage occlusion with the amulet device: to tug or not to tug?[J]. J Interv Card Electrophysiol, 2021, 61(1): 199-206. doi: 10.1007/s10840-020-00821-y
[17] Faletra FF, Saric M, Saw J, et al. Imaging for patient's selection and guidance of LAA and ASD percutaneous and surgical closure[J]. JACC Cardiovasc Imag, 2021, 14(1): 3-21. doi: 10.1016/j.jcmg.2019.06.032
[18] Freixa X, Tzikas A, Sobrino A, et al. Left atrial appendage closure with the amplatzerTM cardiac plug: impact of shape and device sizing on follow-up leaks[J]. Int J Cardiol, 2013, 168(2): 1023-1027. doi: 10.1016/j.ijcard.2012.10.031
[19] Sandhu A, Varosy PD, Du CG, et al. Device-sizing and associated complications with left atrial appendage occlusion: findings from the NCDR LAAO registry[J]. Circ Cardiovasc Interv, 2022, 15(12): e012183.
[20] Helal B, Khan J, AlJayar D, et al. Risk factors, clinical implications, and management of peridevice leak following left atrial appendage closure: a systematic review[J]. J Interv Card Electrophysiol, 2024, 67(4): 865-885. doi: 10.1007/s10840-023-01729-z
[21] Mahmoudi K, Galea R, Elhadad S, et al. Computed tomography scan evidence for left atrial appendage short-term remodeling following percutaneous occlusion: impact of device oversizing[J]. J Am Heart Assoc, 2023, 12(17): e030037. doi: 10.1161/JAHA.123.030037
[22] Garot P. Oversizing TAVR in the low-risk era: is bigger still better?[J]. JACC Cardiovasc Interv, 2021, 14(19): 2170-2172. doi: 10.1016/j.jcin.2021.08.022
[23] Chiang CH, Yeh ML, Chen WL, et al. Apparatus for comparison of pullout forces for various thoracic stent grafts at varying neck angulations and oversizes[J]. Ann Vasc Surg, 2016, 31: 196-204. doi: 10.1016/j.avsg.2015.10.007
[24] Nagumo S, Wakabayashi K, Tsujiuchi M, et al. Clinical impact of undersized-versus oversized-stenting approaches in ST-elevation myocardial infarction[J]. Cardiovasc Revasc Med, 2016, 17(6): 362-368. doi: 10.1016/j.carrev.2016.04.004
[25] Sincos IR, da Silva ES, Belczak SQ, et al. Histologic analysis of stent graft oversizing in the thoracic aorta[J]. J Vasc Surg, 2013, 58(6): 1644-1651. e4. doi: 10.1016/j.jvs.2013.02.005
[26] Taylor JD, Lehmann ED, Belli AM, et al. Strategies for the management of SVC stent migration into the right atrium[J]. Cardiovasc Intervent Radiol, 2007, 30(5): 1003-1009. doi: 10.1007/s00270-007-9109-3
[27] Liu ZN, Zhang JR, Huang J, et al. Small oversized stent graft is associated with increased patency for the treatment of central venous disease in hemodialysis patients[J]. J Endovasc Ther, 2024: 15266028241232921. doi: 10.1177/15266028241232921
[28] 张婷婷, 张玉顺, 万陈, 等. 过大房间隔缺损封堵器对犬术后内皮化的影响[J]. 中华心血管病杂志, 2014, 42(7): 557-560.
[29] Scicchitano P, Gesualdo M, Cortese F, et al. Atrial septal defect and patent foramen ovale: early and long-term effects on endothelial function after percutaneous occlusion procedure[J]. Heart Vessels, 2019, 34(9): 1499-1508. doi: 10.1007/s00380-019-01385-2
[30] 黄曜, 王建铭, 王琦光, 等. 置入房间隔缺损封堵伞的形态对术后头痛的影响[J]. 中华心血管病杂志, 2020, 48(6): 495-499.
[31] 韩丹. 介入封堵治疗房间隔缺损患者并发心律失常的影响因素[J]. 国际护理学杂志, 2022, 41(10): 1755-1758.
-
图(1)
表(5)
计量
- 文章访问数: 739
- PDF下载数: 86
- 施引文献: 0