
-
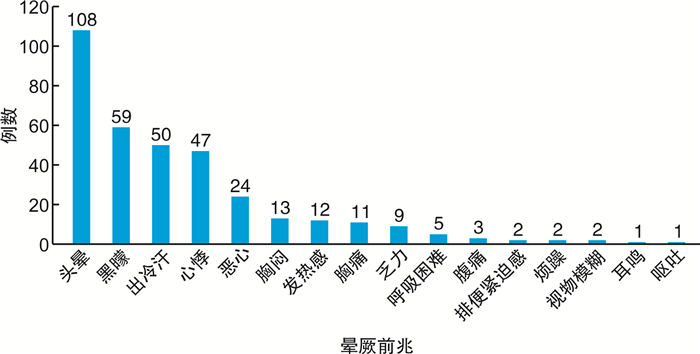
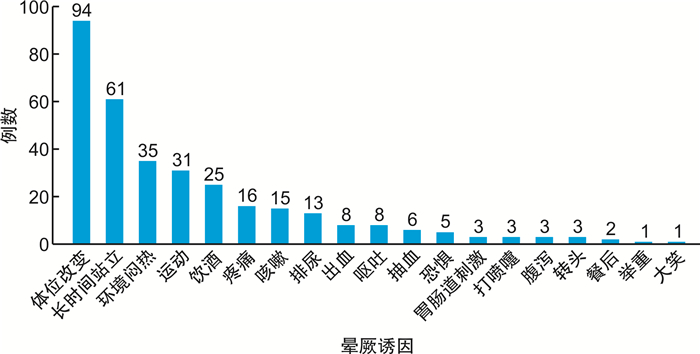
摘要: 目的 对单中心晕厥患者临床资料进行分析,探讨晕厥患者的临床特点和预后情况。方法 本研究共纳入研究对象505例,包括2019年1月—2021年1月于内蒙古医科大学附属医院门诊或住院诊断为“晕厥”的患者363例,以及通过纸质版和电子版问卷进行调查,收集调查问卷142例。收集患者的临床基线资料,通过电话随访方式,在第1、4、8和12个月收集数据,对其疾病进展和发生的事件进行1年的监测。结果 ① 505例患者中,男257例(50.9%),平均年龄(55.52±17.23)岁,平均首次发作年龄(52.30±19.45)岁,中位发作次数1.00次(1.00,2.00)次。333例(65.9%)有诱因,以体位改变最常见,347例(68.7%)有晕厥前兆,最多见的为头晕。②最常见的晕厥为反射性晕厥222例(44.0%),反射性晕厥中最常见的为血管迷走性晕厥183例(82.4%);第二常见的为心源性晕厥123例(24.4%),以缓慢性心律失常晕厥最常见58例(47.2%);其次为直立性低血压晕厥22例(4.4%)。最终有138例(27.3%)晕厥原因仍未明确。③反射性晕厥患者中存在晕厥前兆的比例高于不明原因晕厥患者的比例,差异有统计学意义(P < 0.001)。反射性晕厥患者存在晕厥诱因的比例显著高于心源性晕厥和不明原因患者的比例,差异有统计学意义(P < 0.001)。④采用logistic回归分析探讨不明原因晕厥的影响因素。结果表明,首次发病年龄偏大,合并脑血管用药者中,以不明原因晕厥居多。在大多数有晕厥先兆、诱发因素和伴发心律失常的患者中,晕厥的病因可以确定。⑤对入选患者进行电话随访,共随访245例(606人次),平均随访时间(8.11±3.46)个月,210例(85.7%)结局良好(未复发),28例(11.4%)晕厥复发,4例(1.6%)因晕厥而摔伤,16例(6.5%)再次就诊于门诊,18例(7.3%)再次住院治疗,4例(1.6%)死亡。心源性晕厥结局良好的比例低于反射性晕厥和不明原因晕厥,差异有统计学意义(P < 0.05),心源性晕厥再住院的比例高于反射性晕厥和不明原因晕厥,差异有统计学意义(P < 0.001)。结论 本中心研究结果表明,反射性晕厥最常见,多数存在前兆和诱因,预后较好。第二常见的是心源性晕厥,以缓慢型心律失常晕厥为主,存在诱因和前兆较少,预后较差。首次发病年龄偏大,合并脑血管用药者中,以不明原因晕厥居多。在大多数有晕厥先兆、诱发因素和伴发心律失常的患者中,晕厥的病因可以确定。对于晕厥患者需积极寻找原因,根据危险分层不同制定个体化治疗方案。Abstract: Objective To analyze the clinical data of patients with syncope in a single center and to discuss the clinical characteristics and prognosis of syncope patients.Methods A total of 505 subjects were included in the study, including 363 patients diagnosed with "syncope" in the outpatient or inpatient department of the Affiliated Hospital of Inner Mongolia Medical University from January 2019 to January 2021. A total of 142 questionnaires were collected through the questionnaire survey in both paper and electronic versions. Clinical baseline data were collected for enrolled patients and data were collected over the telephone at 1, 4, 8, and 12 months, followed by 1-year monitoring of disease progression and events.Results ① Among the 505 patients, there were 257 males (50.9%), with an average age of (55.52±17.23) years, an average age of the first episode of(52.30±19.45) years, and the median number of episodes 1.00(1.00, 2.00)times. 333 cases (65.9%) had predisposing factors, and posture change was the most common. 347 cases (68.7%) had a precursor of syncope, and the most common was dizziness. ② The most common syncope was 222 cases (44.0%) in reflexsyncope and 183 cases (82.4%) in reflexsyncope with vasovagal syncope. Cardiogenic syncope was the second most common in 123 cases (24.4%), and bradyarrhythmia syncope was the most common in 58 cases (47.2%). This was followed by 22 cases (4.4%) of orthostatic hypotension syncope. In 138 cases (27.3%) the cause of syncope is still unclear. ③ The proportion of patients with syncope precursor in reflexsyncope was higher than that of patients with unexplained syncope, and the difference was statistically significant (P < 0.001). The proportion of patients with syncope precipitating factors in reflexsyncope was significantly higher than that of patients with cardiogenic syncope and unexplained syncope, and the difference was statistically significant (P < 0.001). ④ Logistic regression analysis was used to explore the influencing factors of unexplained syncope. The results showed that the older the patient was for the first attack, the etiology of syncope in patients combined with cerebrovascular drugs was not easy to be clear. Patients with syncope precursors and precipitating factors, and patients combined with arrhythmia were more likely to be clear about the etiology of syncope. ⑤ A total of 245 patients (606 person-times) were followed up by telephone. The average follow-up time was (8.11±3.46) months. Among the 210 cases (85.7%) with good results (no recurrence), 28 cases (11.4%) had recurrence of syncope, four cases (1.6%) were injured due to syncope, 16 cases (6.5%) were treated in the outpatient department again, 18 cases (7.3%) were treated in the hospital again, and four cases (1.6%) died. The proportion of cardiogenic syncope with good outcome was lower than that of reflexsyncope and unexplained syncope (P < 0.05), and the proportion of cardiogenic syncope re-hospitalization was higher than that of reflexsyncope and unexplained syncope (P < 0.001).Conclusion The results of the research conducted by our center showed that reflexsyncope was the most common one, where precursors and precipitating factors existed for the most part and the prognosis was good. Cardiogenic syncope, which is mainly caused by bradyarrhythmia syncope, is the second most common one, with fewer inducing factors and precursors and a poor prognosis. For unexplained syncope, the older the first episode is, the patients who are combined with cerebrovascular drugs are not easy to identify the cause of syncope. However, patients who are combined with arrhythmia are more likely to identify the cause of syncope because of syncope precursors and precipitating factors. Patients with syncope should actively seek the cause, and formulate individualized treatment plans according to the different risk strata.
-
Key words:
- single center /
- syncope /
- clinical data
-

-
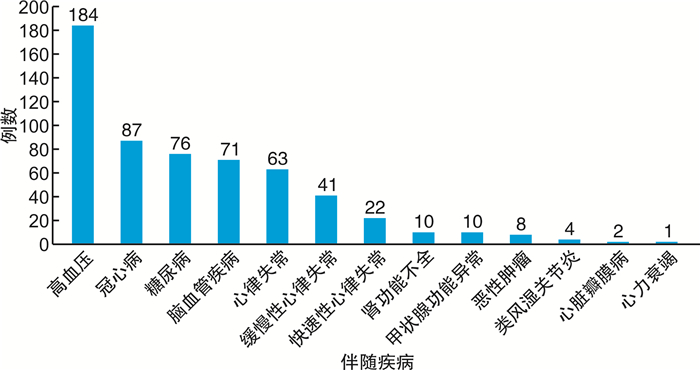
图 3 晕厥患者伴随疾病分布情况
Figure 3. Distribution of concomitant disease in patients with syncope
表 1 晕厥前兆和诱因在不同晕厥中的分布情况
Table 1. Distribution of syncope precursors and precipitating factors in different syncope types
例(%) 项目 反射性晕厥组
(222例)心源性晕厥组
(123例)直立性低血压晕厥组
(22例)不明原因晕厥组
(138例)χ2值 P值 前兆 171(77.0) 86(69.9) 14(63.6) 76(55.1)1)2)3) 19.429 < 0.001 诱因 188(84.7) 65(52.8)1) 18(81.8)2) 62(44.9)1)3) 73.721 < 0.001 与反射性晕厥组比较,1)P < 0.05;与心源性晕厥组比较,2)P < 0.05;与直立性低血压晕厥组比较,3)P < 0.05。采用了Bonferroni校正。  下载: 导出CSV
下载: 导出CSV
表 2 诊断明确晕厥和不明晕厥患者的基本特征
Table 2. Basic features of patients with diagnosed syncope and unexplained syncope
例(%), X±S, M(P25, P75) 项目 明确诊断晕厥组(367例) 不明原因晕厥组(138例) χ2/t/Z值 P值 年龄/岁 53.09±17.78 62.01±13.76 5.969 < 0.001 男性 175(47.7) 82(59.4) 5.527 0.019 首次发作年龄/岁 49.17±20.04 60.62±14.94 6.955 < 0.001 发作次数 1.00(1.00,2.00) 1.00(1.00,3.00) 2.828 0.005 家族史 66(18.0) 16(11.6) 3.010 0.083 前兆 271(73.8) 76(55.1) 16.434 < 0.001 诱因 271(73.8) 62(44.9) 37.333 < 0.001 高血压 123(33.5) 61(44.2) 4.947 0.026 糖尿病 43(11.7) 33(23.9) 11.669 0.001 脑血管病 40(10.9) 31(22.5) 11.101 0.001 冠心病 59(16.1) 28(20.3) 1.249 0.264 心律失常 57(15.5) 7(5.1) 9.913 0.002 缓慢性心律失常 39(10.6) 2(1.4) 11.323 0.001 快速性心律失常 18(4.9) 4(2.9) 0.969 0.325 心脏瓣膜病 2(0.5) 0(0) 0.005 0.941 心力衰竭 1(0.3) 0(0) 0.000 1.000 甲减 5(1.4) 2(1.4) 0.000 1.000 甲亢 0(0) 3(2.2) 4.767 0.029 类风湿关节炎 3(0.8) 1(0.7) 0.000 1.000 肾功能不全 10(2.7) 0(0) 2.561 0.110 恶性肿瘤 6(1.6) 2(1.4) 0.000 1.000 降压药 103(28.1) 60(43.5) 10.899 0.001 降糖药 33(9.0) 24(17.4) 7.066 0.008 脑血管用药 22(6.0) 22(15.9) 12.477 < 0.001 抗抑郁药 4(1.1) 2(1.4) 0.000 1.000 抗心律失常药 29(7.9) 8(5.8) 0.381 0.537
下载: 导出CSV
表 3 影响不明原因晕厥的单因素logistic回归分析
Table 3. Univariate logistic regression analysis on the influence of unexplained syncope
因素 OR值 95%CI P值 年龄 1.03 1.02~1.05 < 0.001 男性 1.61 1.08~2.39 0.019 首次发作年龄 1.04 1.02~1.05 < 0.001 发作次数 0.83 0.72~0.97 0.017 家族史 0.60 0.33~1.07 0.085 前兆 0.43 0.29~0.65 < 0.001 诱因 0.29 0.19~0.44 < 0.001 高血压 1.57 1.05~2.34 0.027 糖尿病 2.37 1.43~3.92 0.001 脑血管病 2.37 1.41~3.97 0.001 冠心病 1.33 0.81~2.19 0.265 心律失常 0.29 0.13~0.65 0.003 降压药 1.97 1.31~2.96 0.001 降糖药 2.13 1.21~3.76 0.009 脑血管用药 2.97 1.59~5.57 0.001 抗心律失常药 0.72 0.32~1.61 0.420 注:因变量:不明原因晕厥组赋值为1,明确诊断晕厥组赋值为0。自变量:年龄、首次发作年龄、发作次数这3个变量均纳入实际数值,其他指标为二分类变量,是赋值为1,否赋值为0。
下载: 导出CSV
表 4 影响不明原因晕厥的多因素logistic逐步回归分析
Table 4. Multivariate logistic stepwise regression analysis of influencing factors of unexplained syncope
因素 OR值 95%CI P值 首次发作年龄 1.03 1.02~1.05 < 0.001 前兆 0.55 0.35~0.88 0.012 诱因 0.33 0.21~0.51 < 0.001 心律失常 0.21 0.09~0.51 0.001 脑血管用药 3.54 1.72~7.28 0.001
下载: 导出CSV
表 5 各类晕厥随访情况比较
Table 5. Comparison of follow-up of various syncope
例(%) 项目 反射性晕厥
组(131例)心源性晕厥组
(59例)直立性低血压晕厥组
(10例)不明原因晕厥组
(45例)χ2值 P值 复发 20(15.3) 5(8.5) 1(10.0) 2(4.4) 4.604 0.203 摔伤 2(1.5) 0 0 0 1.886 1.000 良好 116(88.5) 43(72.9)1) 8(80.0) 43(95.6)2) 12.621 0.006 门诊 10(7.6) 4(6.8) 1(10.0) 1(2.2) 2.144 0.486 住院 4(3.1) 12(20.3)1) 1(10.0) 1(2.2)2) 16.702 < 0.001 心源性猝死 0 2(3.4) 0 0 5.095 0.170 非心血管死亡 1(0.8) 1(1.7) 0 0 2.080 0.715 与反射性晕厥组比较,1)P < 0.05;与心源性晕厥组比较,2)P < 0.05。
下载: 导出CSV
-
[1] 刘文玲, 张海澄, 浦介麟, 等. 晕厥诊断与治疗中国专家共识(2018)[J]. 中华心血管病杂志, 2019, 47(2): 96-107.
[2] Márquez MF, Fragoso JM, Pérez-Pérez D, et al. Polymorphisms in β-adrenergic receptors are associated with increased risk to have a positive head-up tilt table test in patients with vasovagal syncope[J]. Rev Invest Clin, 2019, 71(2): 124-132.
[3] Barbic F, Dipaola F, Casazza G, et al. Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors[J]. J Clin Med, 2019, 8(2): 150. doi: 10.3390/jcm8020150
[4] Quinn J, McDermott D, Kramer N, et al. Death after emergency department visits for syncope: how common and can it be predicted?[J]. Ann Emerg Med, 2008, 51(5): 585-590. doi: 10.1016/j.annemergmed.2007.08.005
[5] Reed MJ. Approach to syncope in the emergency department[J]. Emerg Med J, 2019, 36(2): 108-116.
[6] Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope[J]. Eur Heart J, 2018, 39(21): 1883-1948. doi: 10.1093/eurheartj/ehy037
[7] Ruwald MH, Hansen ML, Lamberts M, et al. The relation between age, sex, comorbidity, and pharmacotherapy and the risk of syncope: a Danish nationwide study[J]. Europace, 2012, 14(10): 1506-1514. doi: 10.1093/europace/eus154
[8] Fischer LM, Dutra JP, Mantovani A, et al. Predictors of hospitalization in patients with syncope assisted in specialized cardiology hospital[J]. Arq Bras Cardiol, 2013, 101(6): 480-486.
[9] Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope[J]. CMAJ, 2016, 188(12): E289-E298. doi: 10.1503/cmaj.151469
[10] Baranchuk A, McIntyre W, Harper W, et al. Application Of The American College Of Emergency Physicians(ACEP)Recommendations And a Risk Stratification Score(OESIL)For Patients With Syncope Admitted From The Emergency Department[J]. Indian Pacing Electrophysiol J, 2011, 11(5): 134-144.
[11] Sutton R, van Dijk N, Wieling W. Clinical history in management of suspected syncope: A powerful diagnostic tool[J]. Cardiol J, 2014, 21(6): 651-657. doi: 10.5603/CJ.2014.0097
[12] Sandhu RK, Sheldon RS, Savu A, et al. Nationwide Trends in Syncope Hospitalizations and Outcomes From 2004 to 2014[J]. Can J Cardiol, 2017, 33(4): 456-462. doi: 10.1016/j.cjca.2016.11.005
[13] 吴瑛, 陈若菡, 孙奇, 等. 单中心晕厥住院患者的病因分析[J]. 中国循环杂志, 2018, 33(6): 596-600. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH201806019.htm
[14] 赵亚楠. 单中心晕厥病因的调查分析[D]. 北京: 北京协和医学院, 2019.
[15] Barón-Esquivias G, Fernández-Cisnal A, Arce-León Á, et al. Prognosis of patients with syncope seen in the emergency room department: an evaluation of four different risk scores recommended by the European Society of Cardiology guidelines[J]. Eur J Emerg Med, 2017, 24(6): 428-434. doi: 10.1097/MEJ.0000000000000392
[16] Safari S, Baratloo A, Hashemi B, et al. Comparison of different risk stratification systems in predicting short-term serious outcome of syncope patients[J]. J Res Med Sci, 2016, 21: 57. doi: 10.4103/1735-1995.187305
[17] 亓晓涵, 王福, 孙慧, 等. 肿瘤与心血管疾病关系的研究进展[J]. 临床心血管病杂志, 2022, 38(7): 585-592. https://lcxxg.whuhzzs.com/article/doi/10.13201/j.issn.1001-1439.2022.07.014
[18] Goldschlager N, Epstein AE, Grubb BP, et al. Etiologic considerations in the patient with syncope and an apparently normal heart[J]. Arch Intern Med, 2003, 163(2): 151-162. doi: 10.1001/archinte.163.2.151
[19] Chen-Scarabelli C, Scarabelli TM. Neurocardiogenic syncope[J]. BMJ, 2004, 329(7461): 336-341. doi: 10.1136/bmj.329.7461.336
[20] Tajdini M, Tavolinejad H, Aminorroaya A, et al. Clinical Associations of Injuries Caused by Vasovagal Syncope: A Cohort Study From a Tertiary Syncope Unit[J]. J Am Heart Assoc, 2023, 12(1): e027272. doi: 10.1161/JAHA.122.027272
[21] Yasa E, Ricci F, Magnusson M, et al. Cardiovascular risk after hospitalisation for unexplained syncope and orthostatic hypotension[J]. Heart, 2018, 104(6): 487-493. doi: 10.1136/heartjnl-2017-311857
[22] Smith A, Perdue M, Vojnika J, et al. The diagnostic yield of implantable loop recorders stratified by indication: "real-world" use in a large academic hospital[J]. J Interv Card Electrophysiol, 2021, 61(2): 303-311.
[23] Shen WK, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines, and the Heart Rhythm Society[J]. Heart Rhythm, 2017, 14(8): e155-e217.
-
图(3)
表(5)
计量
- 文章访问数: 1817
- PDF下载数: 605
- 施引文献: 0